


When will the sudden adult death syndrome (SADS) end?
The excess all-cause mortality remains high even when by June 19, 2023 there are zero COVID-19 deaths per million for these 5 countries.

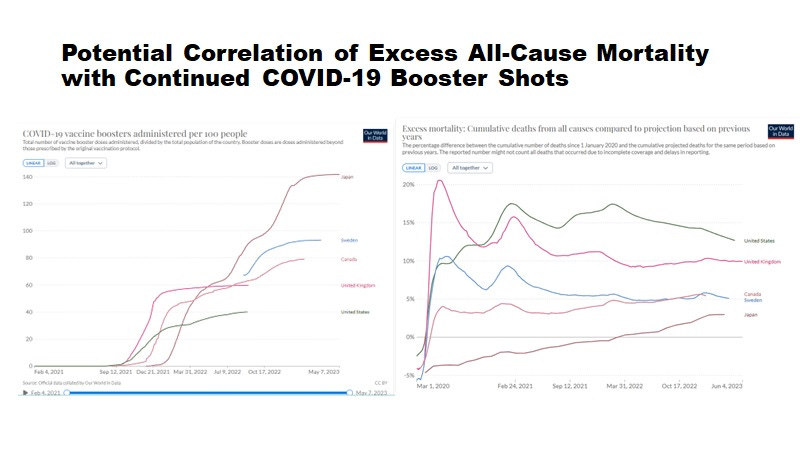
Figure 1. Excess Cumulative Mortality Continues for UK, USA, Canada, Sweden, and Japan Related to Boosting [https://ourworldindata.org/coronavirus]
As shown here in Figure 1 in the Our World in Data graphs, cumulative excess all-cause mortality remains elevated in all 5 countries (UK, US, Sweden, Canada, Japan) despite 0 COVID-19 deaths per million on June 19, 2023 in these countries.
Of the three countries that significantly pushed booster shots beyond September 2022, at least 2 (Japan and Canada) show increasing cumulative excess mortality. This suggests in Canada there may be continued vaccine-associated sudden adult death syndrome cases (SADS) which Dr. Makis tells us is likely to continue.

In the UK, which has been more transparent with mortality data than the other countries, it is clear the continued exposure to boosters has been associated with excess mortality in the different age groups as shown in Figure 2.
Most concerning from Figure 2, is that the excess risk of non-COVID-19 mortality in the 0-24 years-of-age group did not occur until after the vaccines had been administered and which clearly worsened with booster shots. Second, although protection against non-COVID-19 mortality in the 65 plus age group was evident for months December 2020 through May 2021, related to the delay of the administration of the second dose (promoting trained (innate) immunity), and again in January 2022 to April 2022 most likely related to omicron exposures promoting trained (innate) immunity, we see in all age groups by June 2022, the excess mortality continues which is potentially related to booster doses.
According to Irrgang P et al, 2022 [Irrgang P, et al. Class switch toward noninflammatory, spike-specific IgG4 antibodies after repeated SARS-CoV-2 mRNA vaccination. Sci Immunol. 2023 Jan 27;8(79):eade2798. doi: 10.1126/sciimmunol.ade2798], prior natural exposures to SARS-CoV-2 may prevent the conversion of IgG1/3 (which mediate ADE) to IgG4 (which does not mediate ADE see Uversky VN, et al. IgG4 Antibodies Induced by Repeated Vaccination May Generate Immune Tolerance to the SARS-CoV-2 Spike Protein. Vaccines (Basel). 2023 May 17;11(5):991. doi: 10.3390/vaccines11050991).
Thus, post-omicron natural exposures, there may be more conversion of the IgG1/3 to IgG4 in addition to omicron boosting trained innate immunity explaining the benefit of omicron infections on non-COVID-19 mortality.
In contrast, booster shots due to toxicity of the shots (including immediate pulmonary thrombosis associated with injection into the circulation and myocarditis) or due to lingering spike protein causing immunosenescence of macrophages in all age groups [Laderoute MP, submitted] which may lead to increased risk of chronic diseases (namely CVD and so called ‘turbo cancers’) as well as infections in general, might be associated with the enhanced non-COVID-19 mortality shown in Figure 2 (ie. after June 2022).
Figure 2. UK Excess Non-COVID-19 Mortality Percentage by Month by Age Group
[https://twitter.com/OutsideAllan/status/1646813568107511809]
based on data downloaded from: https://www.gov.uk/government/statistics/excess-mortality-in-england-and-english-regions
In the under 25, it appears that vaccination increased the non-COVID-19 mortality risks (largely negative up until Jan 2021) that continues in males.
In the 65 plus, trained immunity (heterologous protection against non-COVID-19 mortality) started in Dec 2020 and lasted until the end of May 2021 (associated with the delay of the second dose in the elders) and then again with Omicron exposures (Jan 2022 to April 2022).
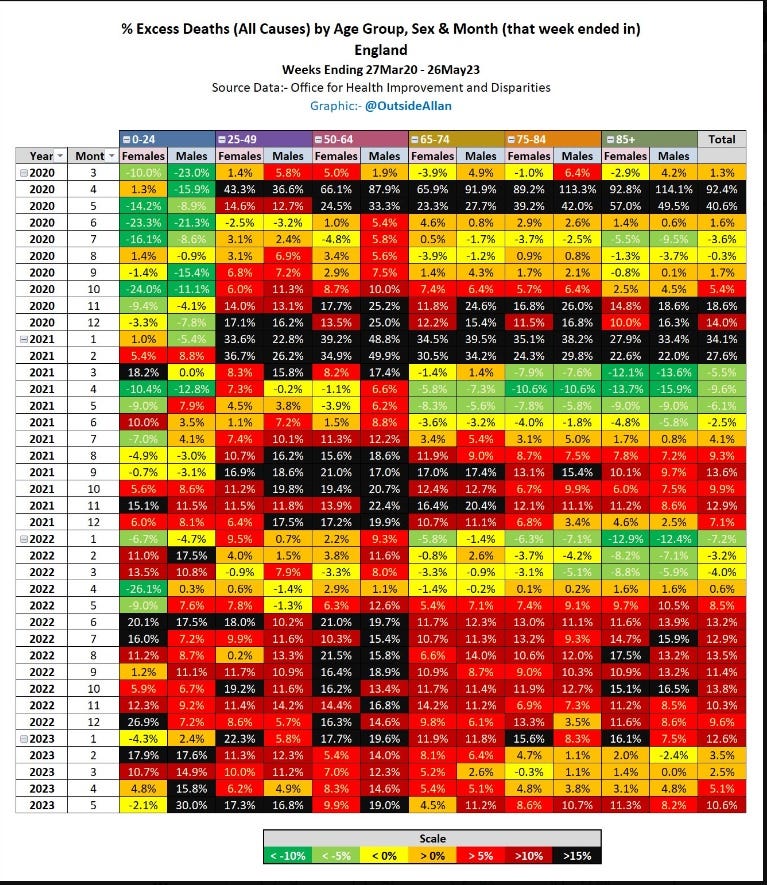
Figure 3. UK Excess All-Cause Mortality Percentage by Month by Age Group
https://twitter.com/OutsideAllan/status/1666901141718720526
based on data downloaded from: https://www.gov.uk/government/statistics/excess-mortality-in-england-and-english-regions
No evidence to suggest vaccination consistently reduced all-cause mortality in any age group. Indeed in the under 25 year olds, vaccination appears to have increased all-cause mortality with increased risks in males that continues.
To illustrate, in a case reported by Walker et al [Walker MR, et al. Characterization of SARS-CoV-2 humoral immune response in a subject with unique sampling: A case report. Immun Inflamm Dis. 2023 Jun;11(6):e910. doi: 10.1002/iid3.910.la], initially spike-specific IgG3 was produced to the 2 dose COVID-19 vaccine, which then converted to IgG1. The first booster promoted IgG3 and IgG2. The natural exposure to the Delta variant and then subsequently to the omicron variant were associated with a predominantly IgG4 spike-specific responses although IgG1 was still detected to the wild type virus. Thus, natural exposures after vaccination may favor the conversion of spike-specific IgG isotypes to IgG4 isotypes (which do not inhibit trained immunity via ADE) while booster shots might not.
These phenomena may help explain why repeated booster shots may be detrimental to non-COVID-19 mortality (June 6, 2022 onward in Figure 2) ie., direct toxic effects of the mRNA ‘spike protein’ vaccines (including the notion that spike protein may induce the immunosenescence of macrophages, submitted). Trained innate immunity not only protects against tumors and infections but also non-COVID-19 mortality more generally [Xu S et al, COVID-19 vaccination and non–COVID-19 mortality risk — seven integrated health care organizations, United States, December 14, 2020–July 31, 2021. MMWR Morb Mortal Wkly Rep 2021;70:1520–1524. doi: http://dx.doi.org/10.15585/mmwr.mm7043e2. ; Li W, et al. A single-cell view on host immune transcriptional response to in vivo BCG-induced trained immunity. Cell Rep. 2023 May 30;42(5):112487. doi: 10.1016/j.celrep.2023.112487.].
Indeed, according to the new immunosenscence paradigm (Figure 3) [Laderoute MP. A new paradigm about HERV-K102 particle production and blocked release to explain cortisol mediated immunosenescence and age-associated risk of chronic disease. Discov Med. 2015 Dec;20(112):379-91. ] the inhibition of trained (innate) immunity by vaccine-induced immunosenescence could increase chronic disease risks such as CVD and tumors as well as infections more generally.
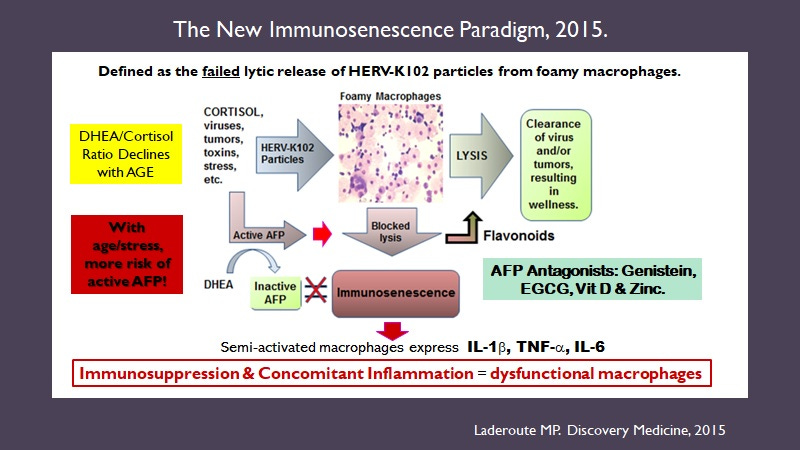
Figure 3. The new immunosenescence paradigm of macrophages.
On a daily basis, Dr. William Makis reminds us of the unexpected or sudden deaths of adults that continues in Canada and throughout the world. However, since most deaths especially sudden deaths are not investigated by autopsy and for spike protein, there is generally no clear substantiation that the vaccines might be causing the deaths.
However, the late Dr. Arne Burkhardt (pathologist) gave a seminar to the Canadian COVID Care Alliance on June 4, 2023 where he discussed SADS. He also discussed how the vast majority of post-vaccination sudden deaths were considered unrelated to vaccination whereas upon autopsy and a second opinion, about 91% were found to be related to COVID-19 vaccination. This outstanding talk was one day before his untimely death for the 79 year old who via autopsies and staining for spike protein versus nucleoprotein proved the COVID-19 vaccines were causing deaths including ‘sudden adult death syndrome’.
Of 31/75 deaths involving cardiac failure, 15 were peri-myocarditis and 16 were microangiopathies with stenosis and dissection, all which stained for spike but not nucleoprotein.
Dr. Arne Burkhardt provided evidence beyond a reasonable doubt that the COVID-19 vaccines are causing deaths including unexpected deaths and cause unknown.
In his discussion of SADS, the fact that 1/19 SADS cases involved death in a car and 1/19 while at work, is not very reassuring for travelers. I have and continue to post-pone a flight to western Canada (since 2021) for this very reason.
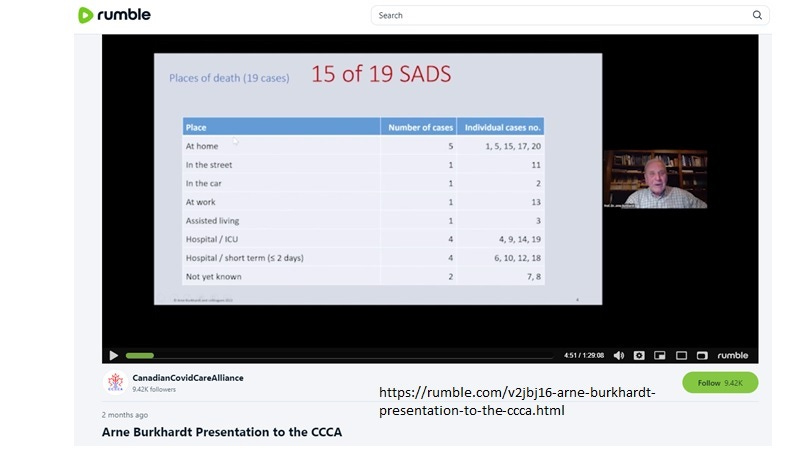
https://rumble.com/v2jbj16-arne-burkhardt-presentation-to-the-ccca.html
He also said that he knew of a severe case of EBV reactivation post vaccination which resulted in a spleen rupture post vaccination.
He also detected an abnormal clot from a blood sample from a 40 year old female marathon runner with unusual perfusion in the feet (the clot developed in the serum upon centrifugation and then standing at room temperature). This was analyzed for proteins. The clots were not fibrin but fibrinogen. There were 137 clot enriched proteins identified one of which was IgM (but no IgG isotypes were detected). This abnormality of the clot formation in the cooled serum occurred 8 months after her last shot. Skin biopsies showed evidence of microangiopathy (at 8 months after her last shot).
Very recently more information on the deaths associated with vaccination was published:
Hulscher N, Alexander PE, Amerling R, Gessling H, Hodkinson R, Makis W, Risch HA, Trozzi M, McCullough PA. A Systematic Review of Autopsy Findings in Deaths after COVID-19 Vaccination. Available at SSRN: https://ssrn.com/abstract=4496137 or http://dx.doi.org/10.2139/ssrn.4496137.
However, the Lancet pre-print was removed by Lancet before it could be viewed by myself 24 hours later.
At this point in time, it is anyone’s guess, when it will be safe to fly again.
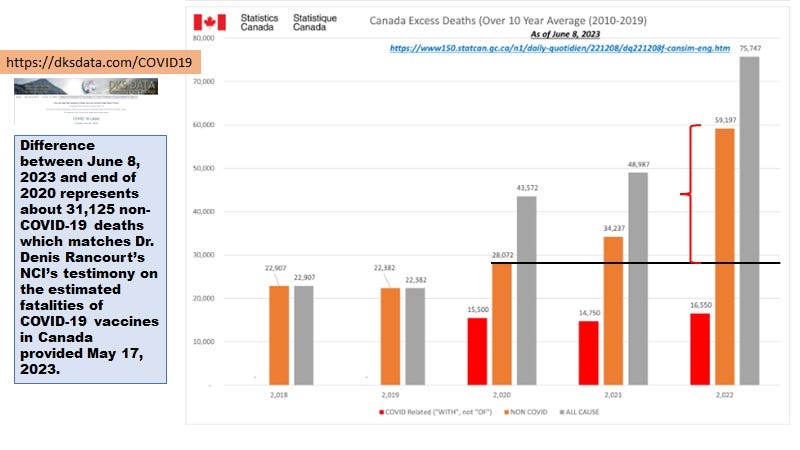
In the meanwhile, in Canada it has been estimated from Statistics Canada website that there have been an excess of 30,000 deaths related to vaccination (excess deaths from end of 2020 to June 8, 2023) which matches Dr. Denis Rancourt’s NCI testimony on May 17, 2023 (see https://rumble.com/v2ohtte-physicist-dr-denis-rancourt-presents-his-findings-on-all-cause-mortality-ot.html).
see https://twitter.com/hervk102/status/1667211796405469194
The five deaths on the submersible Titan on Sunday June 18, 2023 has received more attention and investigation by Canadian government authorities than the over 30,000 Canadians who have met with untimely and often unexpected deaths, where the cause of death is most likely the COVID-19 vaccines. Equally alarming these deadly gene therapy shots (masquerading as vaccines, which they clearly are not) remain on the market and more gene therapy shots are being made for other infectious organisms.
Remember that in the UK from January 2021 to end of May 2022, in the 50 plus population who were ever vaccinated with at least one mRNA COVID-19 vaccine dose (and most with 3 shots by May 31, 2022), there were excess deaths in 1 of every 51 persons vaccinated.
See
Excess Non-COVID-19 Death Counts For the 50+ in the UK, (from January 1, 2021 to May 31, 2022) at 1/51

Table 1. Raw Death Counts in UK from January 1, 2021 to May 31, 2022. From:
Why aren't autopsies mandatory for cases of SADS (with staining for spike versus other viral proteins)? Why weren't autopsies mandatory for all deaths occurring in the vaccinated during the first month of rollout (how else would one distinguish if the gene therapies were or were not killing people)? Why wasn't the mortality data for the first month of the roll out made public for each country? Where is Canada's mortality data (all-cause, non-C19, and C19 mortality) by age, month and stratified by number of doses received? Doesn't the Public Health Agency of Canada know how to conduct surveillance? What kind of public health doesn't perform surveillance? {Compromised, I guess.}
A copy of the Lancet preprint can be found here https://dailysceptic.org/2023/07/06/lancet-study-on-covid-vaccine-autopsies-finds-74-were-caused-by-vaccine-journal-removes-study-within-24-hours/