
Rapidly Elevating EACM in the 0-44 Age Group in Canada in 2023
Can >50 ng/ml of blood Vitamin D3 and Ivermectin Solve This?
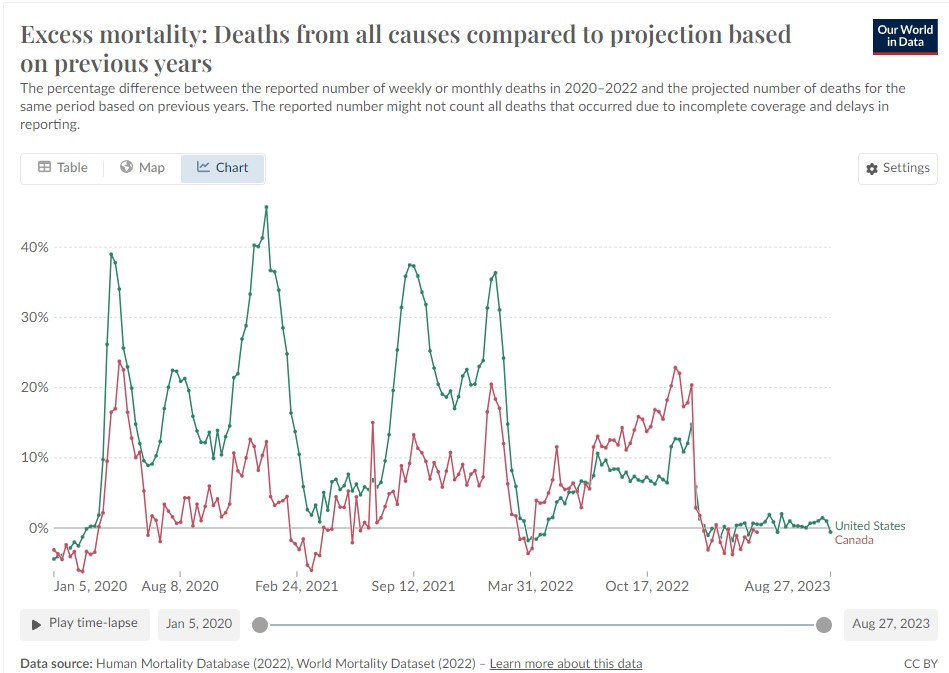
Image 1. Canada vs USA for EACM.
I became a little perturbed when I saw that the excess all-cause mortality was higher for Canada than the USA in 2022. By Feb 1/2, 2022 Canada had 252.13 shots per 100 population and the USA was 203.83. At 90.4 % vaccinated (Canada) and 81.4% (USA) the index was about 228 (boosted) to 166 (incomplete primary).
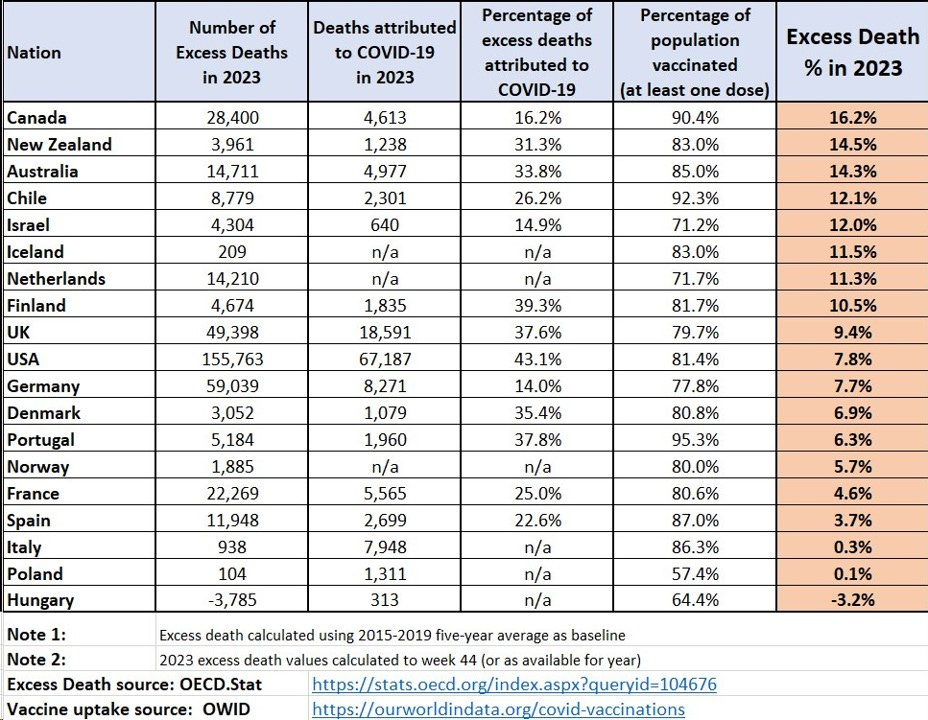
Image 2. OECD Ranking of EACM by Country
For unknown reasons Japan is NOT listed in Image 2. But from Image 3 below, Japan appears to be worse off than Canada for EACM.
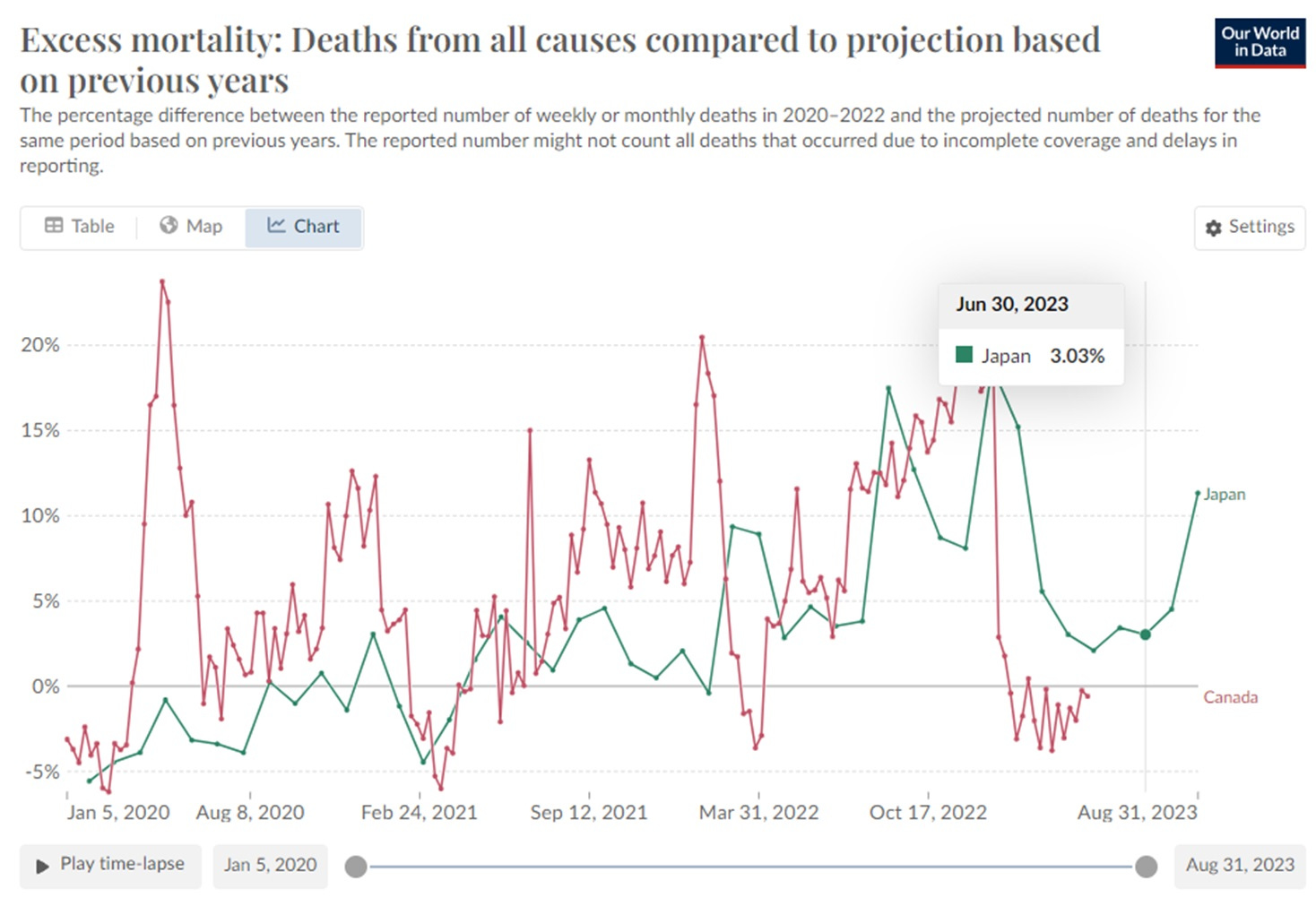
Image 3. EACM Canada Vs Japan
But while the data in Image 3 from ‘Our World in Data’ shows EACM for Canada from Jan 22, 2023 through April 23 2023 under 0, the bulk data at OECD indicates 16.2 %.
This mismatch in data needs explanation.
Drilling down on the dates for the OECD Canadian EACM data, we see that the total resembles the 65 + because the latter group has the highest number of deaths contributing to the total (Image 4).
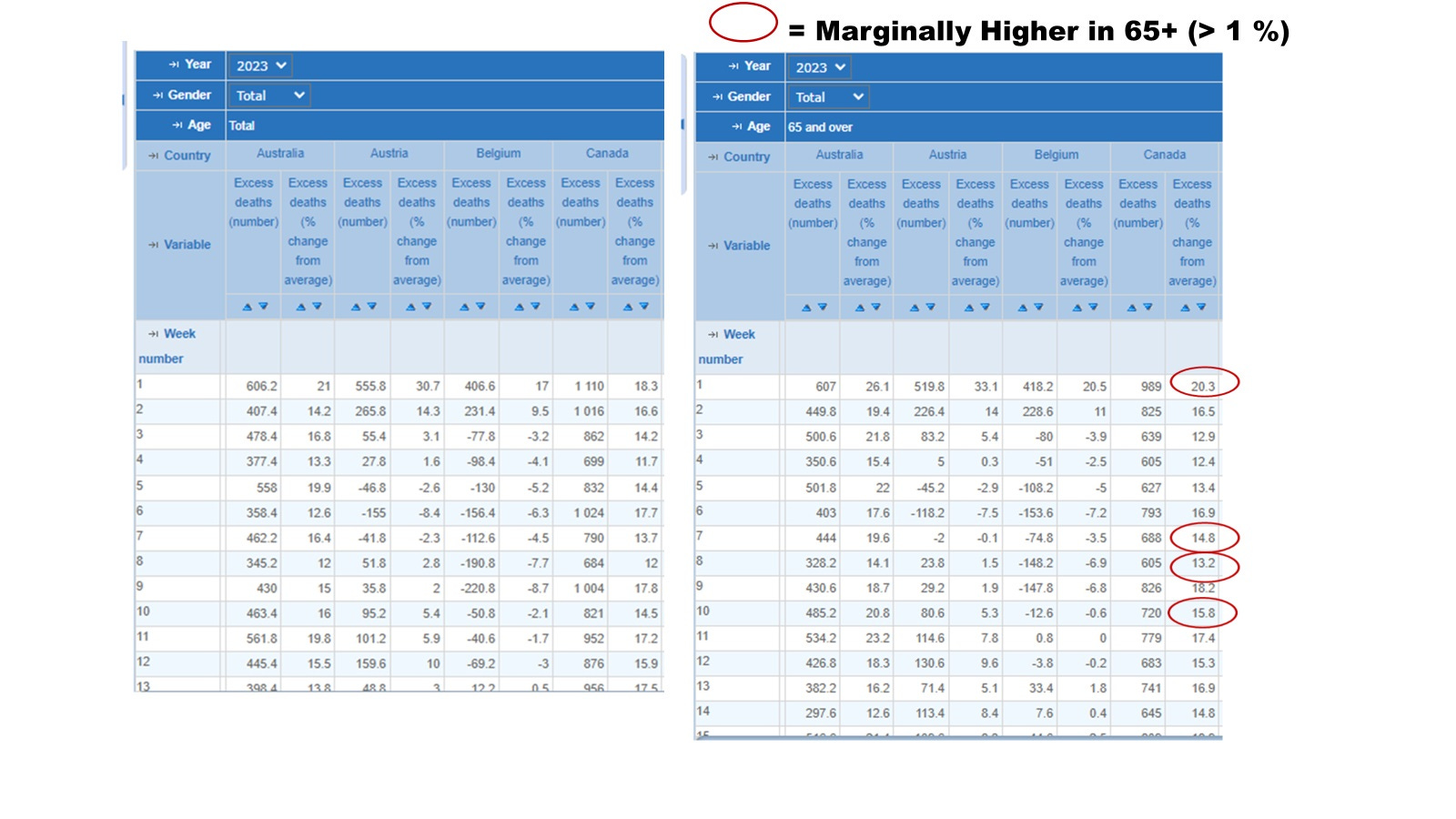
Image 4. The Total For All Ages Resembles the 65 Plus Because most of the Deaths are in this Age Group
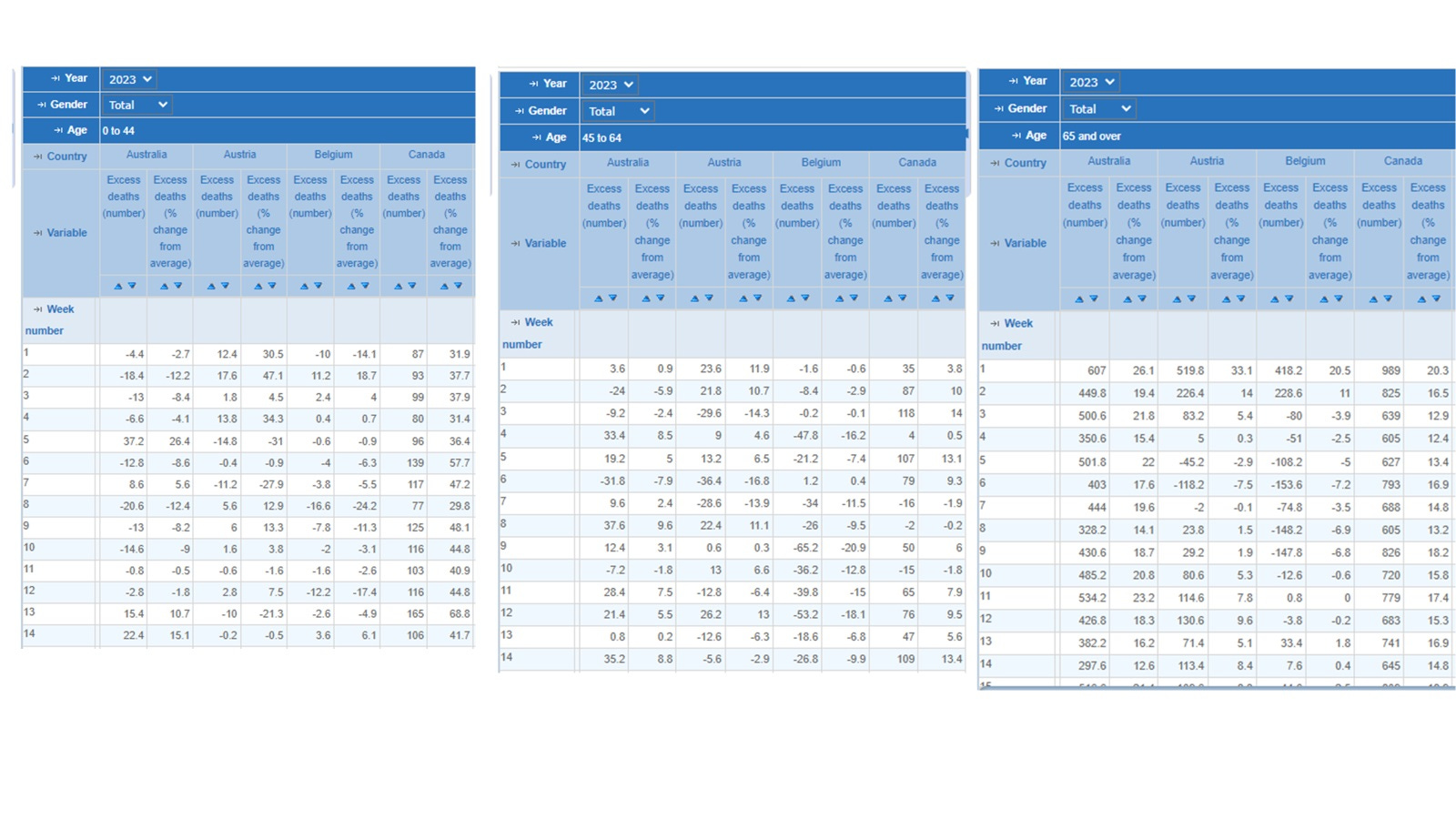
Image 5. EACM Data for First 3 Months of 2023 Shows that
the 65 + have the most all-cause death absolute numbers
the under 45 have the most RELATIVE increases
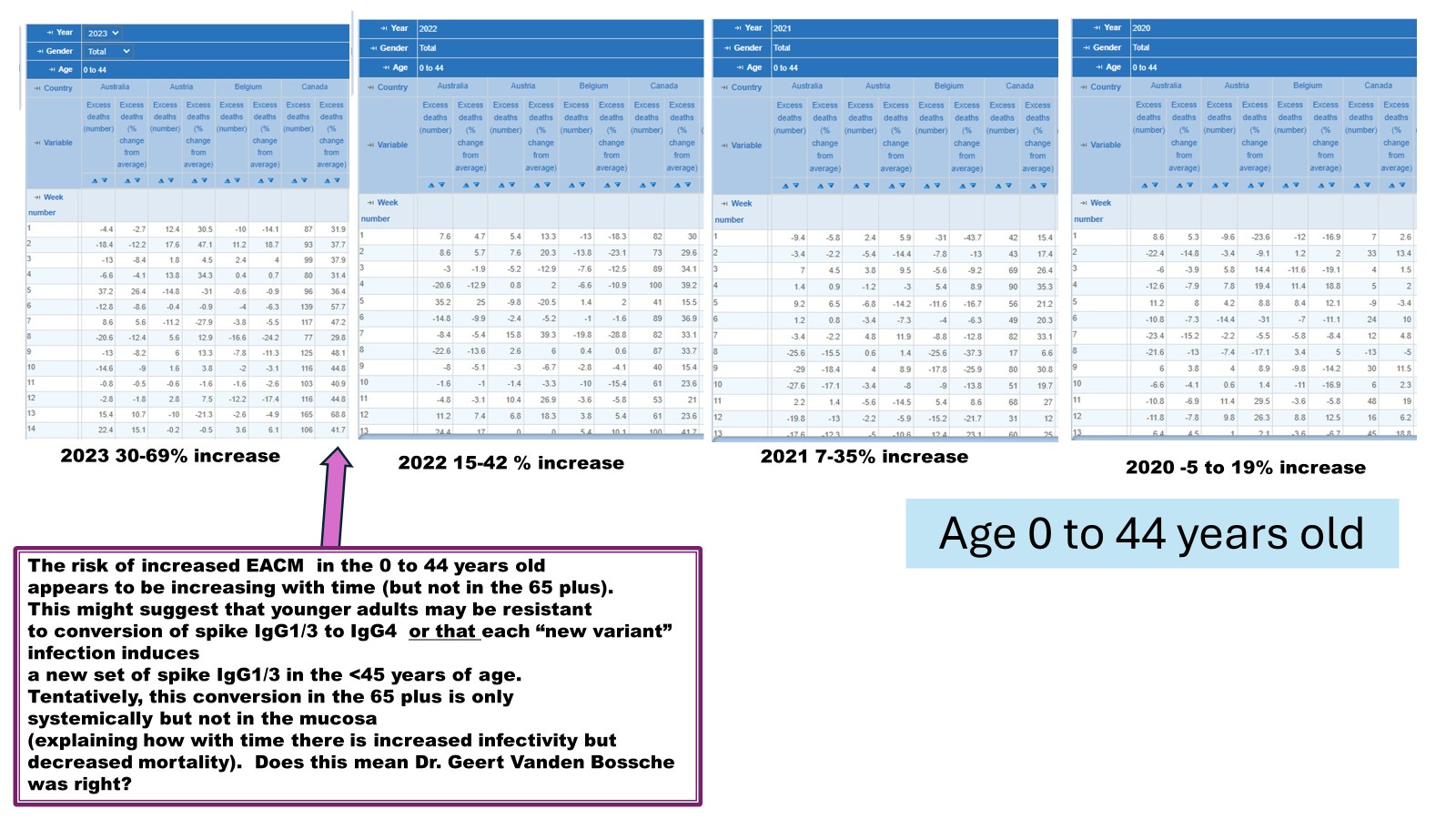
Image 6. EACM Relative Increases Escalating in 2023 in the 0 to 44 years old and for baseline by year since the introduction of COVID-19 mRNA shots.
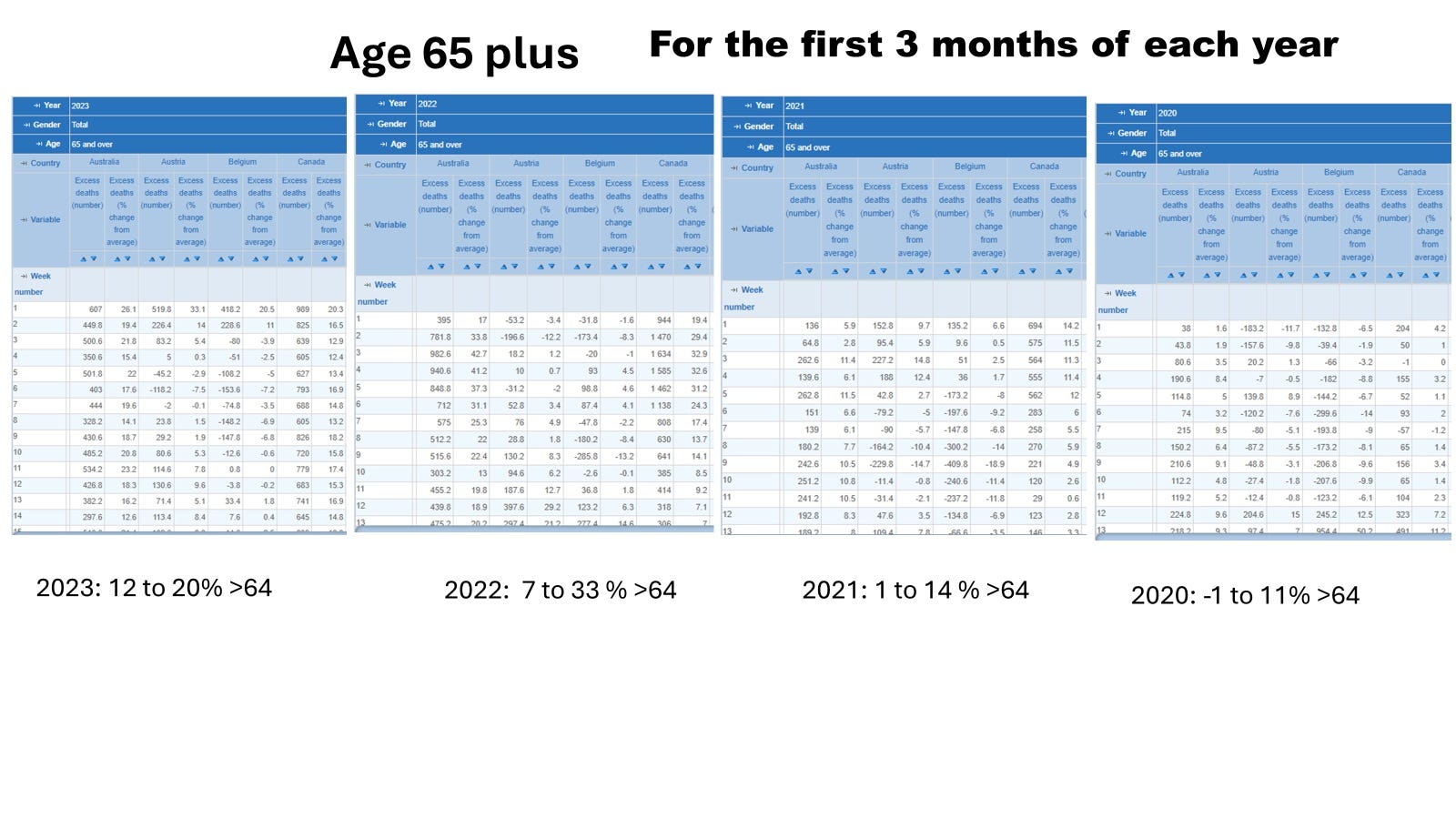
Image 7. EACM baseline elevating per year in the 65 plus age group but not escalating like the 0 to 44 year olds in 2023.
The million dollar question is what is happening here?
Is this because the current SARS-CoV-2 variant has mutated so much that now more recent infections are generating IgG1/3 (once again) which can mediate ADE leading to more severe disease and COVID-19 death?
People who have been vaccinated with the mRNA shots (but not those unvaccinated) maintain IgG1/3 in the upper respiratory tract (URT, which do not appear to transition to IgG4 with the third dose) and so experience heightened (symptomatic) infections when compared with the unvaccinated.
Optimal vitamin D3 unlikely to impact symptomatic infections as it affects only severity and death [Wimalawansa SJ. Infections and autoimmunity-the immune system and vitamin D: a systematic review. Nutrients. 2023 Sep 2;15(17):3842. doi: 10.3390/nu15173842.] ).
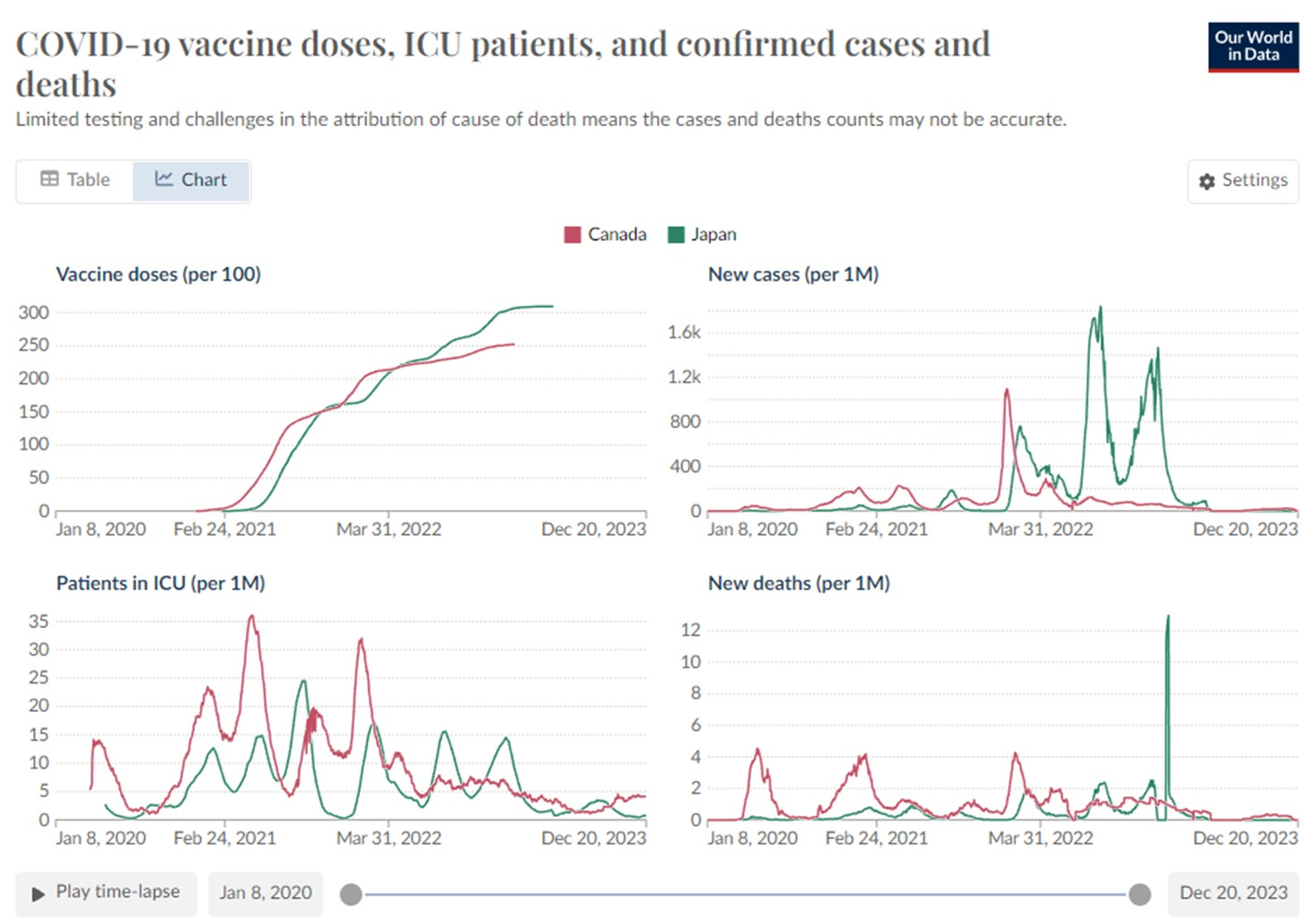
Image 8. COVID-19 Associated Deaths Do Not Appear to be Elevated in Canada in 2023
This might suggest that the elevated EACM in 2023 for Canada may be moreso related to vaccine toxicity/immunosenescence than COVID-19.
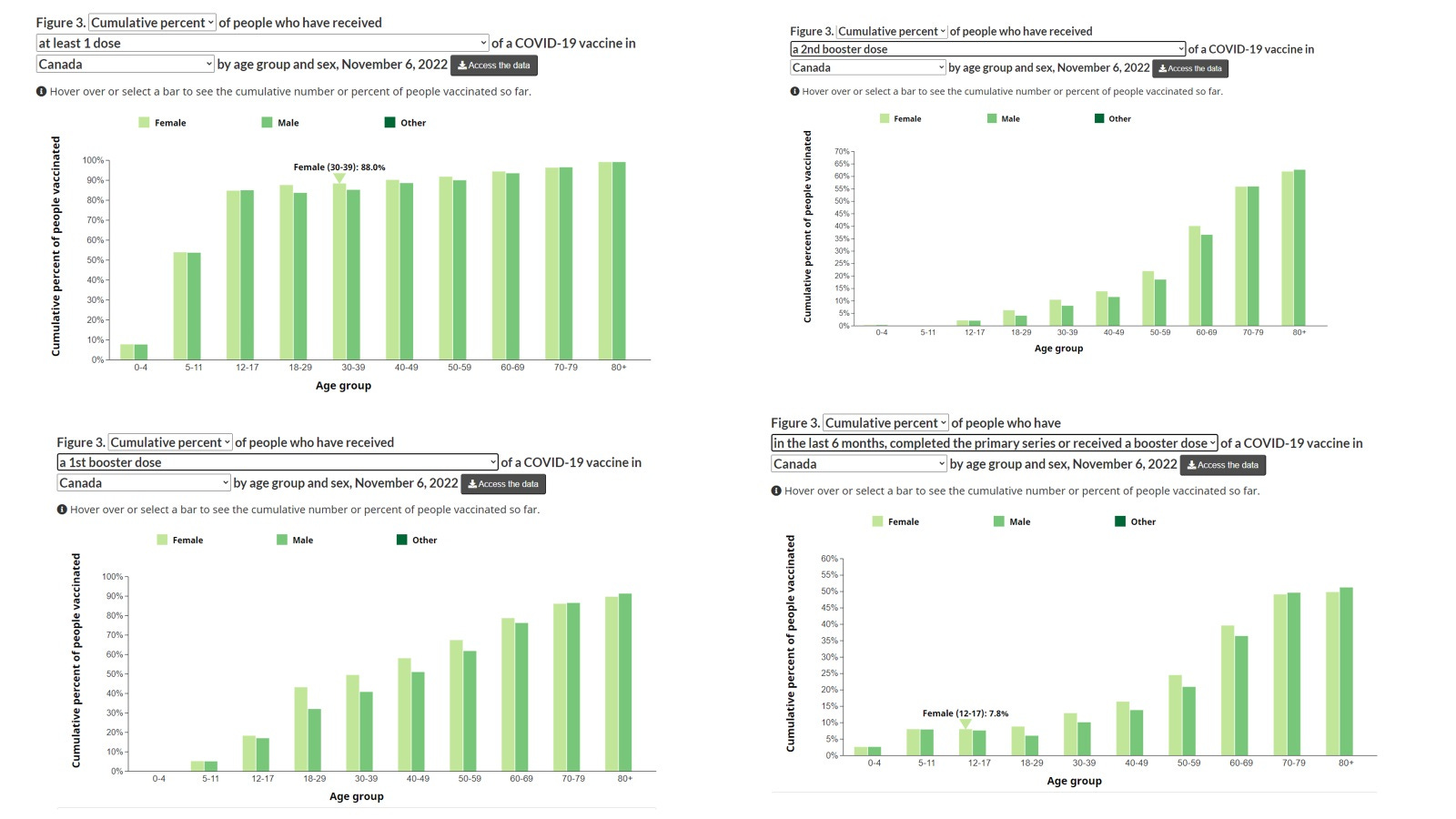
Image 9. About 50% of the <45 received the 3rd dose and about 10% received the 4th dose. Meanwhile 80-90% of the 65 Plus got the third dose and about 50% the fourth dose.
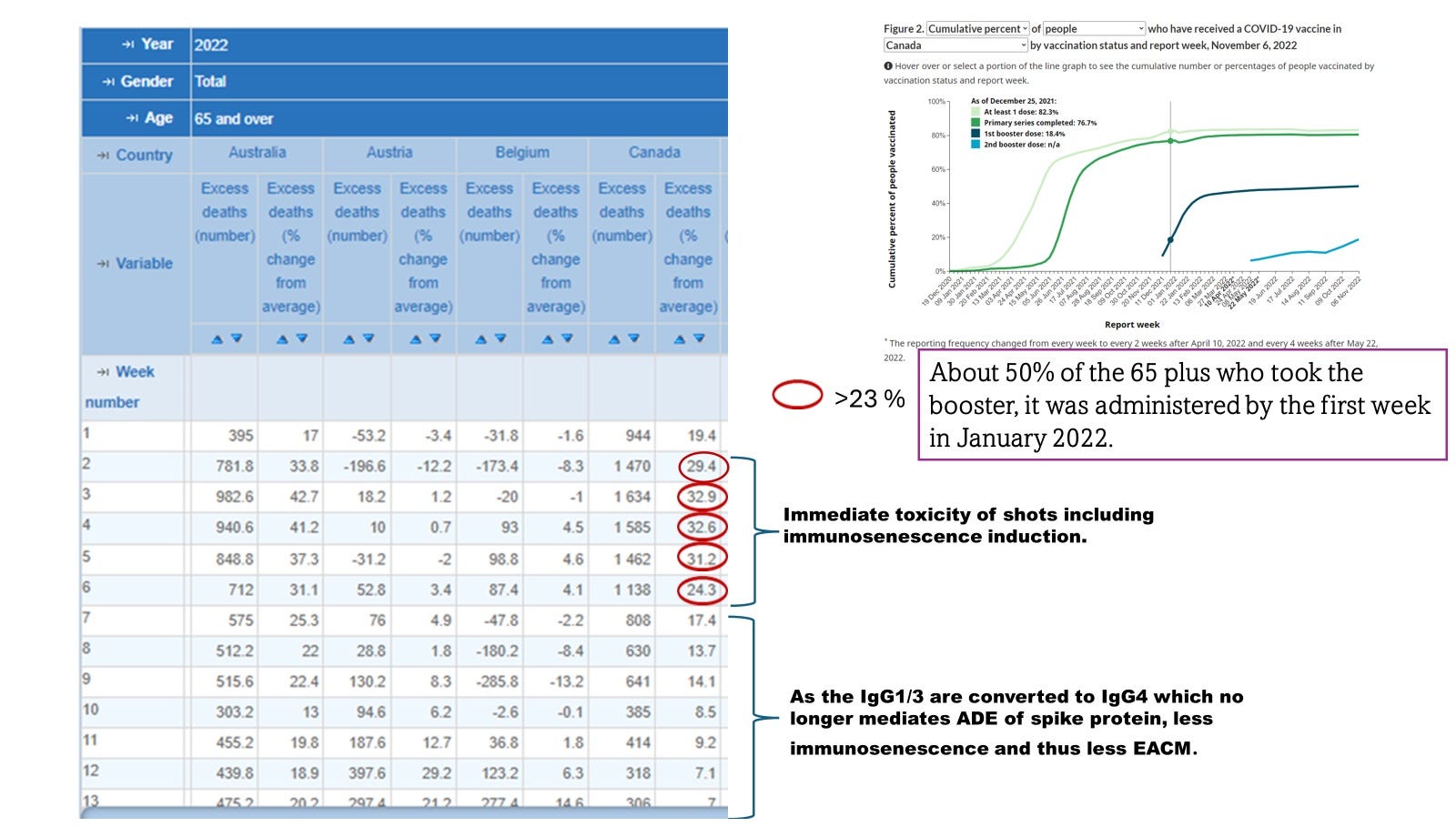
Image 10. The 65 plus Age Group and the Third Dose - A Switch to Less All-Cause Mortality (about 30 % to about 10%).
However by the fourth dose, the EACM was up again in the 65 plus.
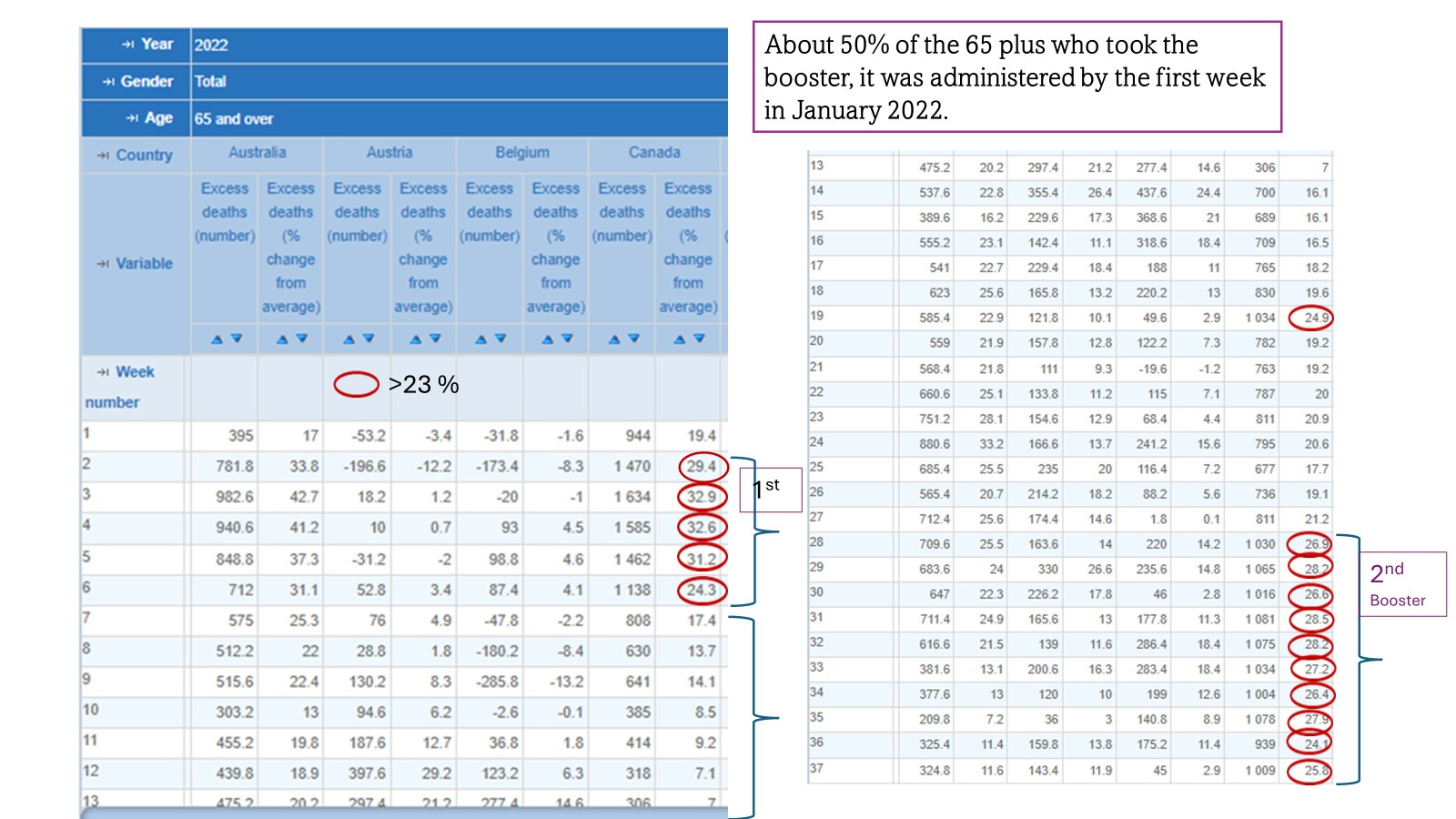
Image 11. The second booster (4th dose) increased EACM in the 65 plus.
A less clear pattern emerged for the under 45 age group for 2022
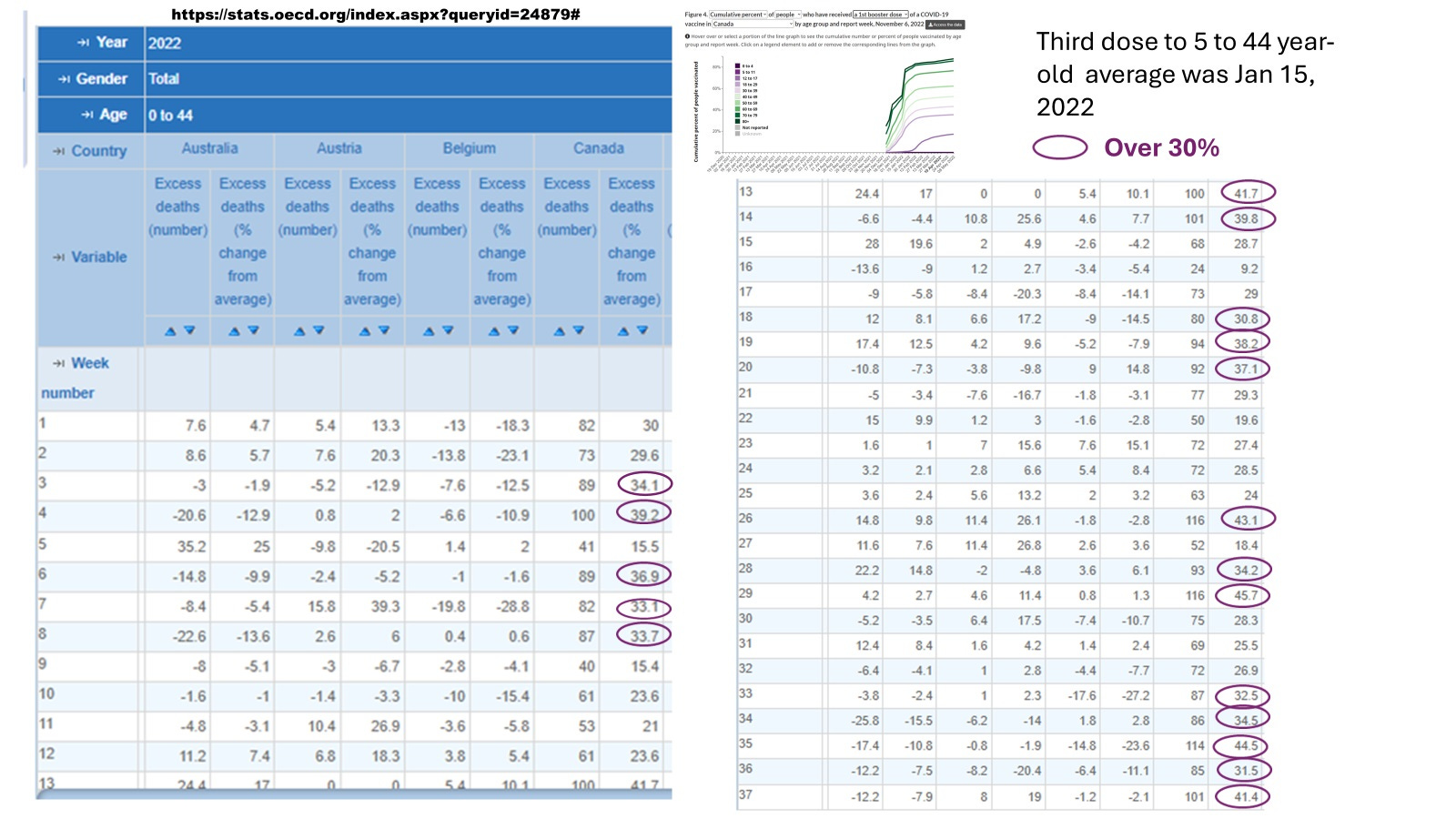
Image 12. Pattern for 2022 for the Under 45 years old less clear.
Perhaps more socializing and exposures to SARS-CoV-2 circulating variants in the under 45 compared with the 65 plus??
Less conversion of IgG1/3 to IgG4 because fewer people took the 3rd dose.
The under 45 might have more exposure to new variants potentially promoting new spike IgG1/IgG3 antibodies promoting ADE and thus higher likelihood of death?
[see https://www.preprints.org/manuscript/202312.0185/v1 for more information on how ADE relates to increased risk of death].
While it is unknown how to deal with the increasing EACM in Canada, the following may or may not help:
To reduce infections place entire population on ivermectin prophylactically (and temporarily wane and contraindicate use of anti-inflammatories such as statins, turmeric, aspirin, and possibly melatonin over 2 mg per night). Works best if entire population is coordinated for at least a month.
To reduce severity and death ensure entire population has vitamin D3 levels well above 50 ng/ml, and takes zinc at 25-50 mg and lysine at 2 g daily.
Clearly world and Canadian experts need to be consulted and protocols drawn up.
It appears that our revered Dr. Geert Vanden Bossche is correct once more. He has already suggested public health agencies will need to broadly prescribe ivermectin… in the very near future.
https://www.voiceforscienceandsolidarity.org/videos-and-interviews/geerts-concern-about-the-new-covid-variant-jn-1
What happens in Japan and Canada over the next few months will hopefully instruct the world on pandemic survival following the mistake of vaccinating during a pandemic (assuming the OECD EACM data are correct).
The innate immunity vaccine being discussed here at https://twitter.com/hervk102/status/1741664933887070357 which activates the HERV-K102 virus anti-virus system in foamy macrophages should block infections (sterilizing immunity) including SARS-CoV-2 and should be useful for those who got 2 or more doses of the mRNA shots. However, if the person has high blood pressure/elevated CRP which are signs of immunosenescence, the effectiveness of this innate immunity vaccine would be reduced. To remedy, ivermectin started before this vaccine, and continued for say a month might help this system get started. Alternatively or additionally, making sure one's blood vitamin D3 levels are well over 50 ng/ml plasma should reduce the risk of death. See my preprint for details.
see also https://twitter.com/AaronKheriatyMD/status/1741371804068012437