

On the Absurdity of the Bio-Pharmaceutical Complex to Do "Anything" to Expand Markets No Matter How Ridiculous
On the Absurdity of the Bio-Pharmaceutical Complex to Do "Anything" to Expand Markets No Matter How Ridiculous
Nothing is more misaligned in our present-day society than publicly supported disease care masquerading as health care.


For relief from hot flashes only HRT is recommended by NAMS despite evidence that it significantly causes cardiovascular disease and breast cancers as published by the 2002 Women’s Health Initiative report (see below). They also recommend AGAINST exercise, yoga, relaxation and various supplements (things known or believed to enhance health).
If we have learnt anything from the COVID-19 pandemic, it is that the interests of Big Pharma to expand its market by perpetuating and in some cases by inducing, disease has reduced our health care system in North America to what would more aptly be referred instead, as ‘disease care’. Health care product regulatory agencies in North America, namely the Food and Drug Administration (FDA) and Health Canada (HC) as well as the public health agencies, the Centers for Disease Control and Prevention (CDC) and the Public Health Agency of Canada (PHAC, separated in 2004 from Health Canada) have been compromised by the interests of Big Pharma for some time now. The ‘Bio-Pharmaceutical Complex’ is a term coined by authors John Leake and Dr. Peter A. McCullough in their recent book “The Courage to Face COVID-19 (2022)”[1]. This term is used to describe the infiltration of Big Pharma objectives within almost all aspects of modern-day medicine and public health and how this corruption adversely affects outcomes by exacerbating disease. The interests of the Bio-Pharmaceutical Complex is to expand the disease market and where more money is more power. The FIVE STEP strategy permitting the Bio-Pharmaceutical Complex to thrive is right out of the tobacco industry and is known as the DISINFORMATION PLAYBOOK:
· The Fake (conduct counterfeit science and try to pass it off as legitimate science),
· The Blitz (harass scientists/clinicians who speak out with results or views inconvenient for industry),
· The Diversion (manufacture uncertainty about science where little or none exists),
· The Screen (buy credibility through alliances with academia or professional societies), and
· The Fix (manipulate government officials or processes to inappropriately influence policy).
Given now that we have social media, I would also add a more recent sixth step namely The Social Media Censoring of Truth (labelling persons, organizations and/or any post, article or video that contradict the Big Pharma propaganda as “misinformation or disinformation” and/or ostracizing them or their messages from social network communities).
To appreciate how the pervasive and profound the corruption of this Bio-Pharmaceutical Complex has become, I think it is very instructive to examine recent examples such as related to the disinformation campaign on the safety and effectiveness of the COVID-19 vaccines.
In October 2021 after generating over 8000 followers (mostly clinicians and medical scientists) on LinkedIn with my COVID-19 scientific commentary articles, I was banned from LinkedIn for posting carefully curated data from official UK government sites (Image 1). This censorship move was allegedly orchestrated by Ian Culbert, the Executive Director of the Canadian Public Health Association in Ottawa[2], who vehemently objected to the notion that the second dose of the COVID-19 vaccines may be associated with an increased risk of death when it involved the delta variant and basically called for my censorship. This variant was a more deadly variant which in fact, was selected by the COVID-19 vaccines [3]. The compiled data in Image 1 suggested that the administration of the second dose of the COVID-19 vaccine might be associated with up to a 1 % increase of death in those who were 50 years of age and older (50 +) and who had contracted the delta variant when compared with those who only had the first dose (Image 1: Table 1). This was also substantiated in part by the demonstration there was also a potential 2% increase in the 50+ population who were hospitalized with the delta variant following the second dose over those who only received the first dose (Image 1: Table 2). It also implied the mortality rate for fully vaccinated patients (ie, with 2 doses) who were 50 years of age and older who were hospitalized involving the delta variant, was about 50%. This is quite a remarkable hospitalization fatality rate!
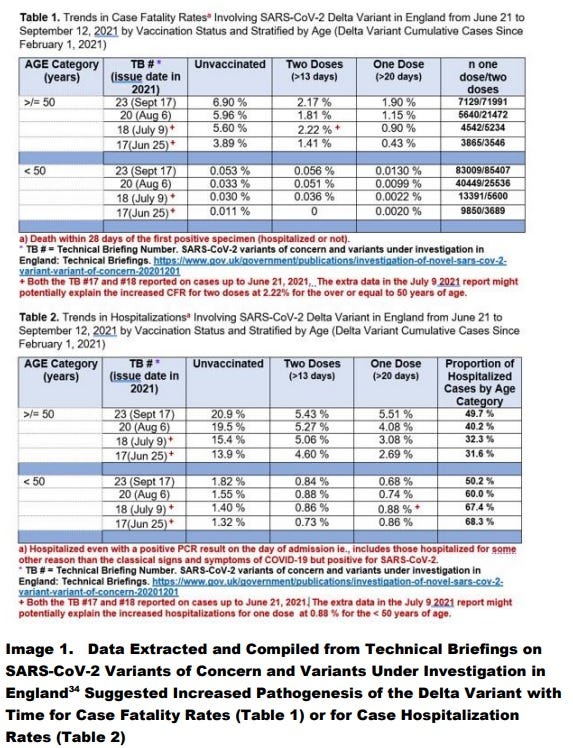
Image 1. Note. Copyright CC-By 4.0.
Interestingly, total UK population-based mortality data released about 9 months later by the Office for National Statistics (ONS) on July 6, 2022 which covered January 1, 2021 to May 31, 2022[4] revealed than in the 50 plus age group, being ever-vaxed (the majority having had 3 gene therapy shots over this time) the excess death rate of the ever-vaccinated over the unvaccinated was 1 in 51 or about 2 % of the ever-vaccinated[5]. Thus, official death statistics later indicated there was INDEED probable cause for concern that the COVID-19 vaccines were COMMONLY associated with death in the 50 + age group (which I had warned about on LinkedIn 9 months earlier). And so, I and others like Dr. Geert Vanden Bosche who were warning about the use of adaptive immunity vaccines and/or risky unproven gene therapy vaccines during a pandemic, were actively censored by the fall of 2021.
This timing may have been due to the release of the infamous report “The Disinformation Dozen” [6] earlier on March 24, 2021 by the Center for Countering Digital Hate. Apparently, emails revealed the White House was colluding by September 2021 with social media giants to censor these and possibly other ‘misinformation spreaders’ online[7].
Note that the data in Image 1 also implies that the first dose which activates trained INNATE immunity involving HERV-K102 activation in foamy macrophages and which is known to provide heterologous protection against all-cause mortality [3], provided better protection for COVID-19 and non-COVID-19 mortality than the full initial series (2 doses) of the COVID-19 vaccines when compared with the unvaccinated. This matches with the extracted UK ONS data [4] raw data compiled by vaccination status shown in Image 2 where we see the only month where the all-cause mortality ratio of ever vaccinated over unvaccinated showed a favorable benefit over risk ratio from January 1, 2021 to May 31, 2022 was in fact, February 2021. This represented a 39% reduction in all-cause mortality (ratio of 0.61). This month was notably different from the others because of those vaccinated by the end of February 2021, 95.6 % had only received the first dose of vaccine but not yet the second (only 531,525 had received the second dose or about 4.4 % of the 11,976,296 vaccinated mostly elders) [reviewed in 3].

Image 2. UK ONS Data Shows only the First Dose of the COVID-19 mRNA vaccine showed Benefit over Risk According to the All-Cause Mortality Algorithm (see discussion in ref. 3]
*Rates are per 100,000 Person-Years, and were re-compiled where all the rates for ever vaccinated were added up to provide totals (as the Ever Vaccinated total deaths reported by the ONS were erroneously undercalculated for unknown reasons). From: ref 3. Note. Copyright CC-By 4.0
It should be blatantly obvious with the UK data that the vaccination protocol with the best hope of saving lives should have restricted immunization to one dose (to only induce trained innate immunity). However, allegedly, the Bio-Pharmaceutical Complex, was able to block the publication of the relevant and properly curated ‘real-time’ mortality surveillance data not only in the UK but globally, including the USA and Canada.
Moreover, there was sufficient UK data by the end of January 2021 (Image 2) to globally rescind the Emergency Use Authorizations (EUAs) of the COVID-19 vaccines by the first week in February 2021, a point further endorsed and repeated by Dr. Peter McCullough [8]. However, for some ‘INEXPLICABLE reason’ this critical surveillance information did not reach the masses to delay indefinitely the second and subsequent doses. Moreover, according to the Helsinki declarations this data must be conveyed in an open and transparent manner so that participants can be fully informed on the risks of experimental therapies such as the COVID-19 vaccines marketed under EUAs. However, the regulatory agencies in cahoots with Big Pharma have been eroding the Helsinki ethics declarations as has been discussed by L. Eggertson published in Canadian Medical Association Journal in 2012.[9]
We can see in Image 2 that May 2021 is when the problem of antibody dependent enhancement (ADE) of SARS-CoV-2 or even high-level spike protein infection into foamy macrophages leading to increased mortality [3] was strongly exacerbated by the second dose in the UK. This followed the putative selection of the delta variant within the fully vaccinated population [3]. The emergence and dominance of the delta variant in the UK occurred in May 2021: namely, the delta variant incidence rates were 4.2%, 18% and 54% on April 26, May 10, and May 24, 2021, respectively [10]. From Image 2, the raw ratios of the excess all-cause mortality risks of the COVID-19 vaccinated over the unvaccinated reached over 10-fold by January 2022 while for non-COVID-19 mortality it reached over 13-fold and for COVID-19 mortality, it reached over 4-fold.
There can be no doubt that the COVID-19 vaccine (in the UK the most commonly used COVID-19 vaccine was the Pfizer-BioNTech mRNA COVID-19 vaccine) was in fact, associated with significant excess mortality. Moreover, there was absolutely, crystal-clear mortality data contradicting the safety and effectiveness (false) narratives of the 2-dose and 3-dose protocols, which should have led to the immediate withdrawal of the Pfizer-BioNTech mRNA COVID-19 vaccine from the global market. Yet for some ‘INEXPLICABLE reason’ the Pfizer-BioNTech mRNA COVID-19 vaccine not only remained on the market but was given biological licences under the name COMIRNATY in the U.S. on August 23, 2021 and on September 16, 2021 in Canada. This is remarkable because COMIRNATY was not a vaccine (offered little or no protection against infectious agents, did not prevent transmission and was associated with increased all-cause mortality) but a gene therapy with a novel lipid nanoparticle requiring more rigorous protocols and extended safety assessment.
As a gene therapy injected product it was strongly anticipated there would be shedding with dire consequences. While not disclosed by the manufacturers, HC or the FDA, an evaluation for the entire UK population revealed shedding to the unvaccinated may have potentially caused more death than SARS-CoV-2 [11].
More problematic was that the Pfizer-BioNTech mRNA vaccine was highly contaminated with DNA[12] and there was no longer term assessment of the risks of genetic modification of the host, nor risks of neurological, cancer, cardiovascular and autoimmune disease. The persistence of the spike protein in the body had not been studied and so vaccinees were led to believe that the vector and spike proteins were only active and expressed for limited amounts of time in the upper deltoid muscle. Follow-up studies established this as lies [13].
It is very clear that the COVID-19 gene therapy shots represent extreme, patently unacceptable risks, and are the most dangerous and toxic products ever witnessed in the history of medicine even as captured by the FDA’s Vaccine Adverse Events Reporting System (VAERS) [12,13]. Most disconcerting is that the gene therapy mRNA type COVID-19 vaccines were found to greatly weaken innate immunity placing the host at increased risk of any and all infections and tumors [12,13]. Furthermore, the problem is that the data strongly suggested the mRNA spike protein targets and promotes immunosenescence of macrophages3 which causes age associated chronic diseases like cancer[14] and particularly including cardiovascular diseases [15].
The products should have been removed from the global market by the first week in February 2021 had the public health agencies been forthright and transparent about releasing pertinent surveillance data in real time. Frankly, some experts have understandably referred to this level of mortality by vaccination as “criminal” if not genocidal.
With time, particularly as witnessed during COVID-19 there was a massive transfer of wealth from taxpayers directly to Big Pharma. For example, $30 billion was paid out by the US government by Dec 7, 2022 for the COVID-19 vaccines[16]. This transfer of money dissolves the middle class and directly further empowers Big Pharma to override government policies and the airwaves with their own agenda. Dissenting views are not tolerated and many genuinely caring clinicians are stripped of their credentials and livelihoods. Tales of adverse event horrors from the COVID-19 vaccines (mandated for travel or employment) as experienced by patients are banned from social media under the guise of ‘misinformation’. Governments are not providing compensation for the lives lost or the incapacitating disabilities relating to their mandating of these gene therapy, Russian-roulette style ‘clot-shots’[17] for travel.
Historically, the Bio-Pharmaceutical Complex exponentially took off when Big Pharma was indemnified in the USA from adverse outcomes of mandated childhood vaccines by the National Childhood Vaccine Injury Act of 1986. By 1999, under the 21 Code of Federal Regulations 202, direct consumer advertising of prescription drugs was made legal in the USA although consumer advertising started as early as May 19, 1983. Only the USA and New Zealand permit advertising of drugs with their primary indication revealed. Nevertheless, in Canada we are now seeing more and more of these commercials but where the viewer is instructed to “ask your doctor about whether the indications are right for you”. It doesn’t matter now if the indication is revealed or not or that many people do not have a family doctor. What is key is that it allows Big Pharma to control media coverage content. The Big Pharma sponsored commercials on Canadian television are seemingly only second in prevalence to gambling site advertisements. Depravity at its best.
In North America the bulk of the cost of review of prescription drugs for marketing is no longer borne directly by the government (taxpayer) but by the company that wishes to profit by its sale. In 1992 the Prescription Drug User Fee Act was introduced for the FDA and Health Canada started charging fees to the manufacturers in 1995. These and other moves I witnessed at the Bureau of Biologics at Health Canada, which was meant to expedite reviews, invariably and perversely resulted in a conflict-of-interest for the reviewer. This essentially means Big Pharma’s objectives including the rushing of reviews become prioritized while issues of safety, purity and effectiveness are relegated to the back burner to the detriment of the health and wellbeing of consumers. Clearly the citizens would be better served if they paid directly upfront for the review rather than later when the hefty costs of prescriptions with questionable safety and effectiveness are absorbed by governments through taxpayer funds.
As mentioned by 2012 various guidance documents worldwide were denouncing if not outright eliminating the need for placebo controlled randomized clinical trials [9]. This meant that Big Pharma could mask serious adverse events because it was being compared to current standards of therapy many never tested against placebo controls. This is how FAKE science is performed by Big Pharma and accepted by regulatory agencies; but first they collude to craft the improved guidelines [9].
We have seen shoddy standards of care for cancer treatments for many decades where in many if not most cases the treatment is worse than the disease, the ever-growing mandated children’s vaccine schedule of questionable usefulness, safety, and effectiveness (and the denial of links to autism and other ailments such as allergies and ADHD, etc.,) where the hopes for a normal independent life are trashed, the cholesterol myth where elevated cholesterol is considered a disease that must be reduced by statins but which instead places the host at higher risk of chronic disease and infections [15], and more recently the COVID-19 pandemic response where the gene therapy shots caused far more morbidity and mortality than the disease itself [5] in the ever vaccinated and possibly the unvaccinated by the shedding of the gene therapy injected products [11].
Some experts put the blame for the 2023 and 2024 closures of emergency rooms and health care crisis (excessive demand) squarely on the mandating of the COVID-19 vaccines. This has apparently resulted in an avalanche of serious sudden disease and chronic disease especially turbo (rapidly advancing) cancers. In addition, there was a voluntary and forced dropout of physicians related to vaccine mandates.
Women’s Health Issues: Menopause
Women’s health issues have not been immune to the ravages of the Bio-Pharmaceutical Complex. Premarin (derived from pregnant mare’s urine) although largely controversial, has been in use as a hormone replacement therapy (HRT) since 1941 [19]. For the longest time HRT was touted as a means to prevent cancers and cardiovascular disease, that is until the randomized controlled clinical trials (RCTs) of Women’s Health Initiative published in 2002 determined the opposite was in fact, the truth[20]. In comparison with placebo, estrogen with progesterone therapy (EPT) was found to increase chronic heart disease, breast cancers, stroke, pulmonary emboli, and cardiovascular diseases, while decreasing the risks of colorectal cancers and hip fractures. There was no significant effect on all-cause mortality over the average of 5.2 years of follow-up indicating the risks outweighed any potential benefits. The total cancer risk was also not significantly different from placebo. In short there was no evidence that the benefits of HRT outweighed the risks.
Perimenopause
During the menopause, there is a discontinuation of estrogen production by the ovaries whereas estrogen and androgens continue to be produced from dehydroepiandrosterone (DHEA) within the adrenal glands. This means there is a change to a lower production of estrogen. In fact, by this time the production of DHEA is already about 60% less than the levels present at age 30. This change may cause certain symptoms of peri-menopause, such as hot flashes and night sweats, the latter associated with poor sleep (the so-called vasomotor symptoms, VMS).
Women have not been exempted from the madness of promoting longer term disease initiation and maintenance by the increasingly powerful Bio-Pharmaceutical Complex that has infiltrated the ranks of the battalions of our health care system including advisory bodies and associations. With Big Pharma at the reins, there has been a growing focus on profit rather than safety, efficacy and purity of biological and pharmaceutical products. Women have been and continue to be hoodwinked into using hormone replacement therapy (HRT) to supposedly improve their health when in fact HRT enhances the risk of disease by the two most common killers of women; cardiovascular disease (CVD) and breast cancer [20]. HRT failed the gold standard of proving sufficient benefits over risk, namely it did not show a statistically significant enhancement of all-cause mortality after 5 years for HRT over placebo. This was clearly demonstrated by the Women’s Health Initiative in 2002.
Nevertheless, the North American Menopause Society (NAMS) continues to recommend HRT (2022) [21], and discourages most other alternative non-hormonal strategies (2023) [22]. Given that exercise may exacerbate hot flashes and night sweats, in a move which paradoxically implies that HRT apparently does not sufficiently diminish the vasomotor symptoms (VSM) of the perimenopause, NAMS has been the first and only organization to recommend against exercise, yoga and relaxation to promote health in women! It just doesn’t get more ridiculous than that when the focus is on Big Pharma profit by promoting unhealthy lifestyles to expand the disease market.
Comments on Post-Menopause Treatments in Passing
There are other symptoms associated with post-menopause such as loss of muscle mass, fat accumulation, type 2 diabetes, skin atrophy, memory loss, cognition loss, and the Genitourinary Syndrome of Menopause which covers vulvovaginal atrophy, vaginal dryness, painful sex (dyspareunia) and stress incontinence. The late Dr. Fernand Labrie of Quebec City, Quebec CANADA marketed a product called Intrarosa which is prasterone (DHEA) made by chemical modification of a plant compound and showed it suitable for reversing vulvovaginal atrophy and dyspareunia at 6.5 mg per vaginal ovules. Studies indicated it raised blood levels of DHEA by about 3 ng/ml (Intrarosa Canadian Product Monograph or USA package insert). This increase might be sufficient to prevent or reverse immunosenescence in some individuals [14], thereby reducing the age associated risks of infectious agents, tumors, and chronic diseases like cardiovascular disease [14,15]. This is turn potentially could lead to enhanced longevity with less morbidity and enhanced wellness, although this needs to be directly investigated and validated.
It may well be that the highly revered late Dr. Fernand Labrie who held Ph.D. and M.D. degrees was steadfastly resistant to the influence of the Bio-Pharmaceutical Complex.
REFERENCES
[1] Leake J, McCullough PA. The Courage to Face COVID-19. Preventing Hospitalization and Death While Battling the Bio-Pharmaceutical Complex. Counterplay Books, 2022, Dallas, Texas, USA, pp286.
[2] https://www.cpha.ca.
[3] Laderoute, M. Antibody Dependent Enhancement (ADE) of Infection into Macrophages Validates the Importance of HERV-K102 Particle Production for Pandemic Preparedness. Preprints 2023, 2023120185. https://doi.org/10.20944/preprints202312.0185.v1.
[4] https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/deaths/bulletins/deathsinvolvingcovid19byvaccinationstatusengland/deathsoccurringbetween1january2021and31may2022
[5] Laderoute MP. Excess Non-COVID-19 Death Counts for the 50+ in the UK (from January 1, 2021 to May 31, 2022) at 1/51. https://hervk102.substack.com/p/for-the-50-in-the-uk-excess-deaths. [https://hervk102.substack.com/publish/posts/detail/104712689].
[6] https://counterhate.com/research/the-disinformation-dozen/
[7] https://childrenshealthdefense.org/defender/facebook-files-biden-censor-disinformation-dozen/
[8] McCullough, Peter: at U.S. Sen. Ron Johnson Roundtable Discussion. COVID-19 Vaccines: What they are, how they work, and possible causes of injuries. December 7, 2022.
https://twitter.com/SenRonJohnson/status/160050489272825037
. https://rumble.com/v1ze4d0-covid-19-vaccines-what-they-are-how-they-work-and-possible-causes-of-injuri.html.
[9] Eggertson L. Helsinki doctrine under review. CMAJ. 2012 Nov 6;184(16):E827-8. doi: 10.1503/cmaj.109-4295.
[10] https://ourworldindata.org/explorers/coronavirus-data-explorer?
[11] Laderoute MP. February 18, 2024.

[12] Mead MN, Seneff S, Wolfinger R, Rose J, Denhaerynck K, Kirsch S, McCullough PA. COVID-19 mRNA Vaccines: Lessons Learned from the Registrational Trials and Global Vaccination Campaign. Cureus. 2024 Jan 24;16(1):e52876. doi: 10.7759/cureus.52876.
[13] Seneff S, Nigh G, Kyriakopoulos AM, McCullough PA. Innate immune suppression by SARS-CoV-2 mRNA vaccinations: The role of G-quadruplexes, exosomes, and MicroRNAs. Food Chem Toxicol. 2022 Jun;164:113008. doi: 10.1016/j.fct.2022.113008.
[14] Laderoute MP. A new paradigm about HERV-K102 particle production and blocked release to explain cortisol mediated immunosenescence and age-associated risk of chronic disease. Discov Med. 2015 Dec;20(112):379-91.
[15] Laderoute M. The paradigm of immunosenescence in atherosclerosis-cardiovascular disease (ASCVD). Discov Med. 2020 Jan-Feb;29(156):41-51.
[16] https://www.kff.org/coronavirus-covid-19/press-release/covid-19-vaccines-could-cost-billions-of-dollars-more-each-year-if-the-federal-government-ends-its-bulk-purchasing-program/.
[17] Atyabi SMH et al. Relationship between blood clots and COVID-19 vaccines: A literature review. Open Life Sciences 2022; 17: 401–415. https://doi.org/10.1515/biol-2022-0035.
[18] Byrne P, Demasi M, Jones M, Smith SM, O'Brien KK, DuBroff R. Evaluating the Association Between Low-Density Lipoprotein Cholesterol Reduction and Relative and Absolute Effects of Statin Treatment: A Systematic Review and Meta-analysis. JAMA Intern Med. 2022 May 1;182(5):474-481. doi: 10.1001/jamainternmed.2022.0134. See lay summary at https://theconversation.com/benefits-of-statins-may-have-been-overstated-new-study-175557, and a case study at https://nationalpost.com/health/a-vascular-surgeon-explains-why-he-ditched-statin-drugs-for-more-meat-and-less-sugar-and-lowered-his-cholesterol-in-the-process. Interestingly for the evaluation of all-cause mortality in the meta-analysis involving over 66300 participants in each arm, the absolute relative risk reduction of 0.8% was NOT statistically significant (p=0.11), whereas the relative risk reduction at 9% was statistically significant (p=0.01).
[19] Kohn GE, Rodriguez KM, Hotaling J, Pastuszak AW. The History of Estrogen Therapy. Sex Med Rev. 2019 Jul;7(3):416-421. doi: 10.1016/j.sxmr.2019.03.006.
[20] Rossouw JE, Anderson GL, Prentice RL, et al. Risks and benefits of estrogen plus progestin in healthy postmenopausal women: Principal results from the Women's Health Initiative randomized controlled trial. JAMA. 2002;288(3):321–333. doi: 10.1001/jama.288.3.321
[21] https://www.menopause.org/docs/default-source/professional/nams-2022-hormone-therapy-position-statement.pdf.
As a side note another Canadian doctor Dr. Mark Patry has just released his story of how he discovered a safe and effective solution to hot flashes of the perimenopause in a new book on Amazon [https://www.amazon.ca/Unravelling-Menopause-Mark-Patry-ebook/dp/B0CV97CBJ4/ref=sr_1_1?]. Not only do I recommend the book but I recommended the treatment. It worked for me!!!
Oh Dr. Marian. I hadn't yet gotten to your own response to this--just in reading the "Menopause Society" (how utterly embarrassing--such a personal matter) recommendations, I noted right away that the treatment options which cost nothing were dismissed, and only those options from which some agency could make a buck were encouraged. ??? What a joke. My mother took HRE back in the early 70's. I have no idea why--we didn't discuss such things then--that I even know that she did is actually a bit surprising. I wouldn't have ever considered such drugs, and, to his credit, my physician, who had been caring for my health (I use those words judiciously) since I was 28 years old, never once suggested it. Perhaps because he had known me from before I was even a first-time mother. Grateful I am to have been under his care for 41 years; pity he decided to leave his practice five years ago, as he had told me that he intended to remain for quite some time more.