


Must be Disinformation (Hearsay) Due to Lack of Substantiating Data
How to Tell IF Media or the Government is Gaslighting You on the COVID-19 Vaccine Risks...Even IF You Are NOT VACCINATED

The trust index seems paradoxically… untrustworthy.
In this AP news article TO FACT-CHECK INFORMATION on May 6, 2021, an infectious disease clinical trial expert Dr. Kathleen Mullane at the University of Chicago is insinuating only the extremely dumb would believe in the possibility that there is some form of shedding of the overexpressed spike protein from the vaccinated to the unvaccinated from the gene therapy shots that have been promoted as COVID-19 vaccines. From the above it seems Dr. Mullane has herself never heard of vesicles/exosomes or even HERV-K102 particles (Image 1) that transmit proteins, lipids, miRNA and mRNAs extracellularly (so who is the dummy now?) [1]. Clearly she has not read the FDA guidance (FDA-2014-D-0852 of August 2015) on shedding for gene therapies and its requirements for initiating and pursuing clinical trials which was published in 2015 [2].
I don’t believe for a minute that Dr. James A Thorp would agree that “we know it really doesn’t affect fertility at all”. Rather he would say and provide data supporting the claim ”we know it REALLY DOES (adversely) affect fertility and pregnancy outcomes” [3].
Image 1. Natural production of PROTECTOR HERV-K102 particles in lipid body negative M1-like proinflammatory foamy macrophages (release is by lysis). From Laderoute et al, 2007; 2015 [4,5].
Bogus fact-checking aside by Facebook, YouTube, the AP, etc. one should always look for supporting data and not hearsay when so-called self-professed fact-checkers make claims.
There has been considerable discussion that menstruation cycles have been disrupted by vaccination, including in households in cohabitating women who did not get vaccinated.
Dr. Pierre Kory and a Midwestern Doctor [6] recently requested details of situations where potentially recent vaccinees may have shed spike protein or the COVID-19 gene therapy vectors to a non-vaccinated person.
Dr. Kory has posted a summary of his findings on the FLCCC website [7], and talked about his findings February 10, 2024 on the American Thought Leaders as interviewed by Jan Jekielek [8] and February 16, 2024 on the Jeff Dornik Show as interviewed by Jeff Dornik [9].
HERE I am reporting evidence which I think strongly substantiates the claim of clinically significant shedding because here the data is from the entire UK population and it involves the outcome of DEATH in the vaccinated and death in the unvaccinated.
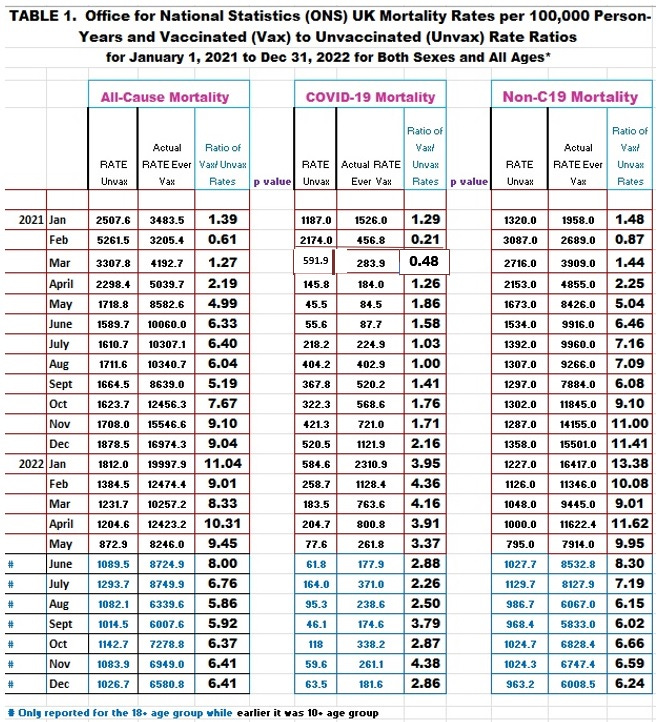
The main mortality rate data (rates per 100,000 person-years) for the vaccinated verses non-vaccinated by all-cause mortality, COVID-19 mortality and non-COVID-19 mortality has been compiled from the UK Office for National Statistics (ONS) data released July 6, 2022 covering the 10+ UK population [10] and with a second report released 2023 covering the 18+ UK population [11].
I have talked about this data (Table 1) and how it shows the COVID-19 vaccines failed the all-cause mortality test for benefit over risk [12] except for February 2021 when about 95 % or more elders had only received the first dose that does not induce the dangerous spike specific IgG1 and IgG3 antibodies.
For more information on why the IgG1/3 spike antibodies are so dangerous, please see a recent review [13].
So bearing in mind Dr. Kory’s request for stories or information on shedding, I thought well, generally, one would expect the ratio of non-COVID-19 to COVID-19 mortality rates in the vaccinated to peak around the time of vaccination due to the well known toxicity of the mRNA vaccines.
If there was any significant shedding to the unvaccinated, one might predict peaks of non-COVID-19 mortality (increased due to shedding) over COVID-19 mortality that would be temporally associated with the peaks in the vaccinated.
So here is the raw data that was used to calculate the non-COVID-19 / COVID-19 mortality rate ratios (Image 2).
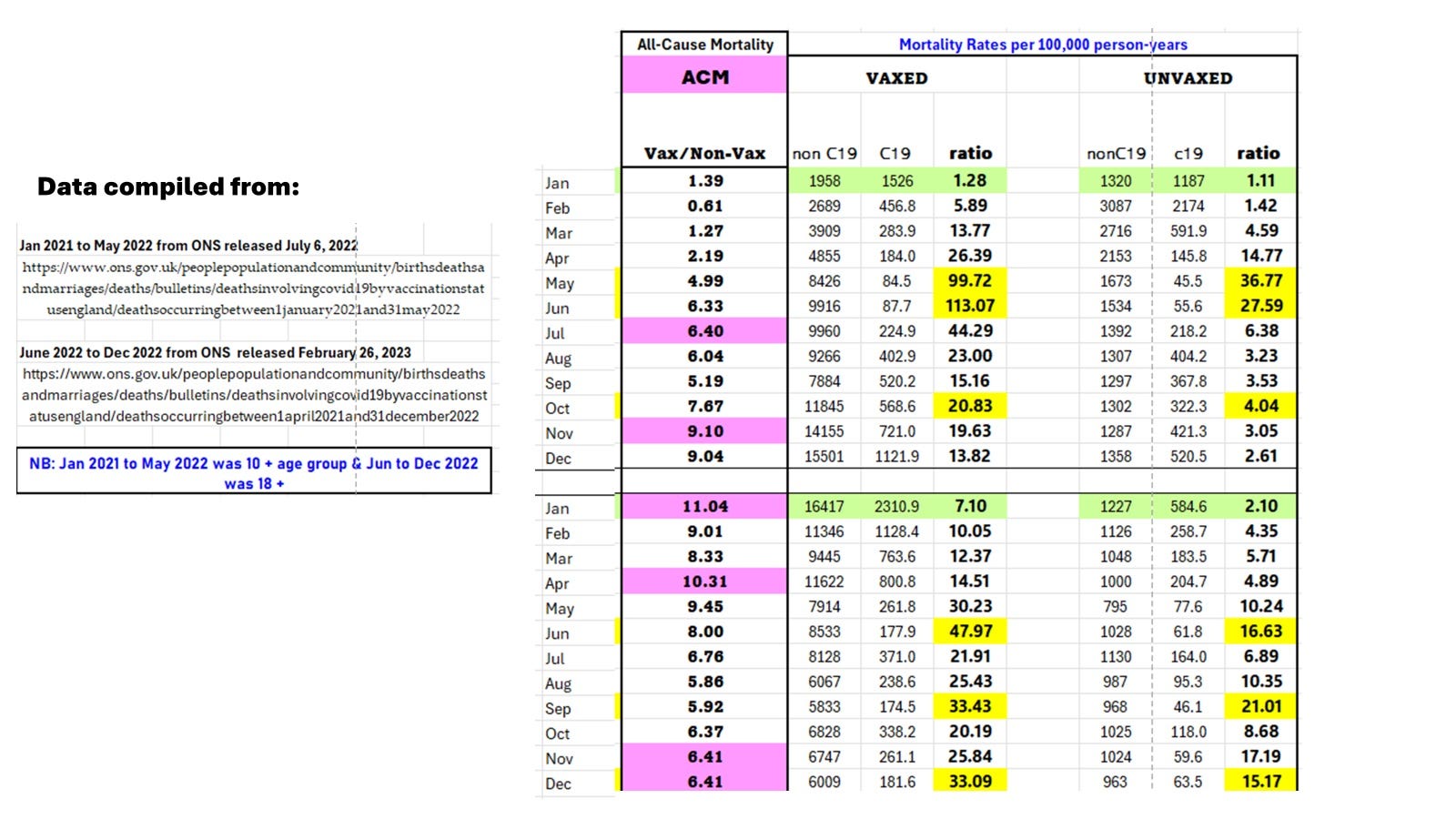
Image 2. Mortality rate ONS data from UK used to calculate the non-COVID-19 to COVID-19 mortality rate ratios separately for the Ever Vaccinated (VAXED) and the Unvaccinated (UNVAXED).
We do see a co-ordination of the timing of the peaks and nadirs (lowest levels) between the VAXED and UNVAXED, consistent with the spreading of the toxic substance from the vaccinated to the unvaccinated. With the exception of February 2021, in all months examined, the rate of NON-COVID-19 mortality was significantly higher in the vaccinated over the unvaccinated as expected as the proximity to higher doses was much higher in the vaccinated.
The all-cause mortality ratio of the VAXED over the UNVAXED reveals mortality was more pronounced in the vaccinated reflecting the vaccine toxicity.
In the UK the vast majority of vaccines used pertained to the Pfizer-BioNTech’s mRNA BNT 162b2 gene therapy shot. Since most of the deaths occur in the elderly it would also be useful to zero in on the time at which the 65 to 75 year olds were vaccinated in the UK (representing the ages where all-cause mortality may be not only common but perhaps more sensitive to outside influences).
If we examine the timing of vaccination in the elderly, we see a tight association with timing of mass vaccination in the elderly with the Non-COVID-19/COVID-19 mortality ratio peaks for the vaxed and unvaxed as shown in Image 3. The worst was in May and June 2021 associated with the induction of the dangerous spike specific IgG1/3 and involving the selection of the delta variant which was known to be more pathogenic.
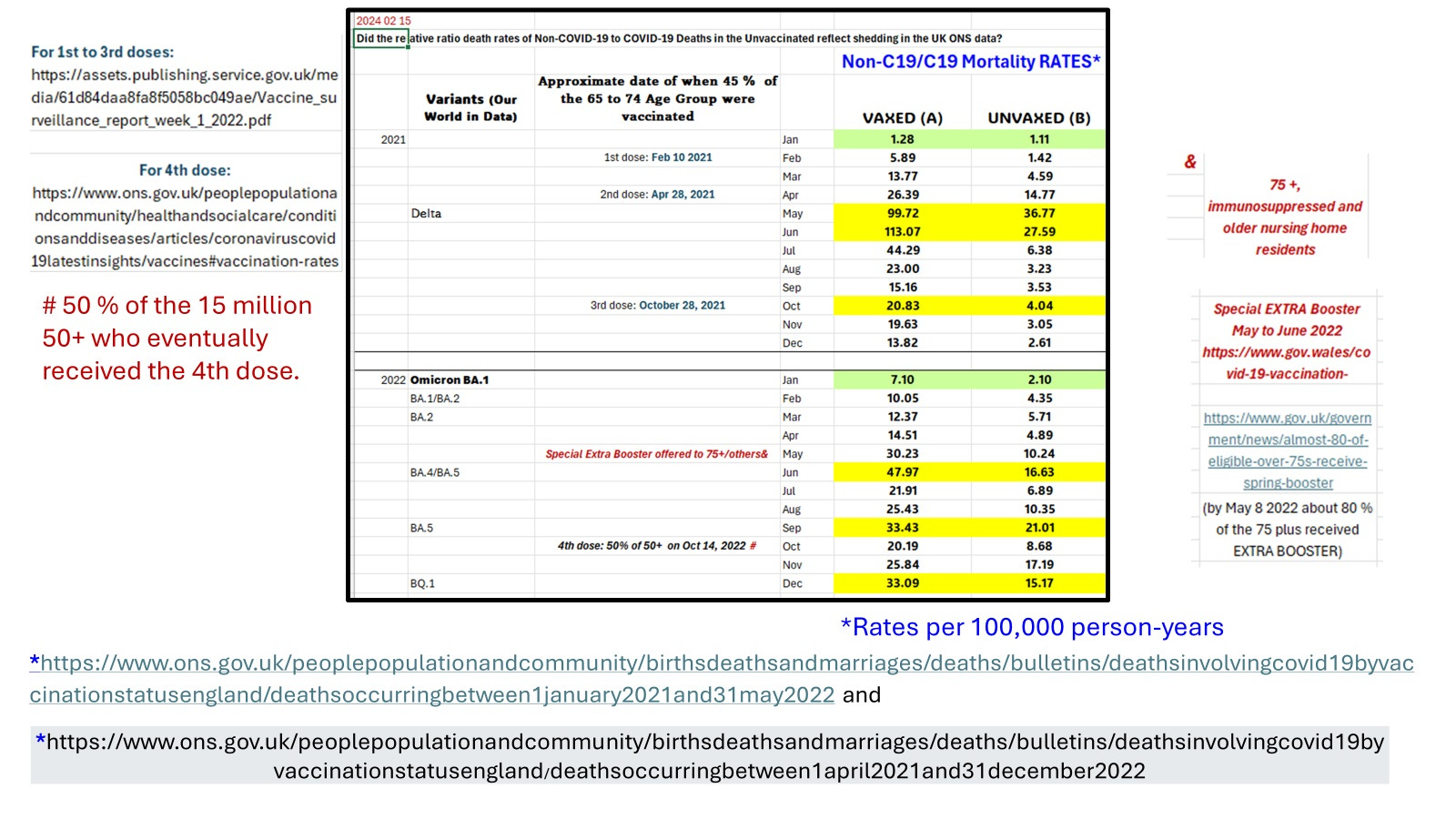
IMAGE 3. Peaks of toxicity in the unvaccinated appear to be temporally associated with peaks of toxicity in the vaccinated (albeit at lower levels).
We know from several studies that the third dose of the COVID-19 mRNA vaccine causes the conversion of the dangerous spike-specific IgG1/3 antibodies to non-dangerous IgG4 (which does not contribute to antibody dependent enhancement of infection into macrophages [13]) [14-18]. Accordingly we see less toxicity associated with the third dose late October 2021, interestingly for both the vaccinated and the unvaccinated.
These results suggest the toxicity of spike protein +/- LNP was exacerbated in the presence of spike-specific IgG1/3 implying the antibodies targeted these toxins to the macrophage. This raises the possibility that the antibodies to spike were also being transmitted with the shedding. Interestingly, Dr. Kory used high levels of antibodies to spike as a surrogate marker of exposure to shed vaccine in the non-vaccinated [9] such as spouses.
Omicron was very infectious and less pathogenic with far less, lower respiratory tract infection. It was believed to have originated from the common house mouse. It induced considerable amounts of negative excess all-cause mortality implying in certain individuals (probably favoring the unvaccinated) that trained innate immunity (of macrophages) was induced which provided heterologous (non-specific) protection against all-cause mortality. This process may have resulted in the nadirs in Image 3 in January 2022 for both the VAXED and UNVAXED.
Shedding may have caused more deaths than SARS-CoV-2 in the Unvaccinated in the UK
In Image 4 an attempt is made to determine if the rate of mortality in the unvaccinated that might be ascribed to shedding exceeds the rate of mortality due to COVID-19. For this the nadir of non-C19 death rates of 795 for May 2022 (Image 2) is subtracted from each of the monthly non-C19 rates.

Image 4. Monthly estimates of the relative mortality rates comparing deaths potentially associated with shedding to those caused by COVID-19 for the UK ONS data for 2021 to 2022.
We see in Image 4 that 2021 was about 3.9-fold more dangerous than 2022 for putative shedding to the unvaccinated which resulted in death.
In the unvaccinated, over the period of January 1, 2021 to December 31, 2022, the average monthly non-COVID-19 excess mortality (above a background nadir to account for other background causes of death) was 569.4 per 100,000 person-years and the average COVID-19 mortality was 348.8 per 100,000 person-years. Clearly the non-COVID-19 mortality which reflects pathology due to shedding from the vaccinated, exceeded the rate of deaths associated with COVID-19.
This is a stunning observation that shedding may have caused significantly higher rates of non-COVID-19 death when compared with COVID-19 deaths in the unvaccinated.
SUMMARY AND CONCLUSIONS:
Dr. Peter McCullough recently remarked that myocarditis and/or sudden death could unexpectantly occur two years after being vaccinated. In these individuals it may be due to exposure to shed vaccine from the recently vaccinated.
Dr. William Makis has remarked that cases of sudden death may relate to being recently vaccinated. The data shown here that equally possible is that the person was exposed to the recently vaccinated, so it becomes a mute point whether the person who died was recently vaccinated or not.
The level of deadly gene therapy contagion in the UK unvaccinated population is not inconsequential and likely was at a level that exceeded the risk of death caused by SARS-CoV-2.
Those that approved and/or facilitated the use of the deadly gene therapy shots and those who mandated such interventions must be held responsible. All mRNA gene therapy shots should in my opinion be globally banned indefinitely. All construction of facilities to produce mRNA vaccines should be stopped and the funds used to pay out the vaccine related deaths and injuries whether vaccinated or not.
One might consider that manufacturers of the gene therapy shots had an obligation to study and report on vaccine shedding required since 2015 by the FDA [2]. Since they allegedly did not (or may have but did not report this data), this may have breached the contract for the sale of the gene therapy shots. Also, calling the gene therapy shots vaccines when they were in fact, gene therapy shots that shed, might be considered evidence of fraud. Restitution might include the return of all monies paid out by governments for the deadly gene therapy shots. This money should be used to compensate for death injuries and disabilities of vaccinated and the unvaccinated.
The failure of the FDA and advisory committees and other regulators worldwide to properly scrutinize the gene therapy shots as gene therapy products and not as traditional vaccines, needs to be subject to an inquiry with criminal prosecution where appropriate. The same can be said for the CDC and their advisory panels that recommended the marketing of the unsafe, contagion products as “a public health measure”. Those who mandated the shots such as for travel or employment, should also be explored for culpability. Finally those who attempted to silence the vaccine injured, scientists, and clinicians particularly the latter by medical licensing boards or heads of universities, and by social media with or without collusion with governments, is considered the most egregious of all, and should in my opinion be investigated for crimes against the constitution.
REFERENCES:
Yu J, et al. Biogenesis and delivery of extracellular vesicles: harnessing the power of EVs for diagnostics and therapeutics. Front Mol Biosci. 2024 Jan 3;10:1330400. doi: 10.3389/fmolb.2023.1330400.
https://www.fda.gov/regulatory-information/search-fda-guidance-documents/design-and-analysis-shedding-studies-virus-or-bacteria-based-gene-therapy-and-oncolytic-products.
Thorpe JA, et al. COVID-19 vaccines: The impact on pregnancy outcomes and menstrual function. Journal of the American Physicians and Surgeons Volume 28 Number 1 Spring 2023. [@ThorpMD on twitter]
Laderoute MP, Giulivi A, Larocque L, et al. The replicative activity of human endogenous retrovirus K102 (HERV-K102) with HIV viremia. AIDS. 2007 Nov 30;21(18):2417-24. doi: 10.1097/QAD.0b013e3282f14d64.
Laderoute MP, Larocque LJ, Giulivi A, Diaz-Mitoma F. Further evidence that human endogenous retrovirus K102 is a replication competent foamy virus that may antagonize HIV-1 replication. Open AIDS J. 2015 Dec 7;9:112-22. doi: 10.2174/1874613601509010112.
https://covid19criticalcare.com/reviews-and-monographs/covid-mrna-vaccine-shedding/
https://www.theepochtimes.com/epochtv/dr-pierre-kory-explains-covid-19-vaccine-shedding-5584790?https://covid19criticalcare.com/reviews-and-monographs/covid-mrna-vaccine-shedding/
https://rumble.com/v4drt10-dr-pierre-kory-live-on-the-jeff-dornik-show.html?mref=1wxk5&mc=ehuil
https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/deaths/bulletins/deathsinvolvingcovid19byvaccinationstatusengland/deathsoccurringbetween1january2021and31may2022.
https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/deaths/bulletins/deathsinvolvingcovid19byvaccinationstatusengland/deathsoccurringbetween1april2021and31december2022.
https://hervk102.substack.com/publish/post/104309209.
Laderoute, M. Antibody Dependent Enhancement (ADE) of Infection into Macrophages Validates the Importance of HERV-K102 Particle Production for Pandemic Preparedness. Preprints 2023, 2023120185. https://doi.org/10.20944/preprints202312.0185.v1.
Irrgang P, Gerling J, Kocher K, et al. Class switch toward noninflammatory, spike-specific IgG4 antibodies after repeated SARS-CoV-2 mRNA vaccination. Sci Immunol 2023;8(79):eade2798. DOI: 10.1126/sciimmunol.ade2798.
Yoshimura M, Sakamoto A, Ozuru R, et al. The appearance of anti-spike receptor binding domain immunoglobulin G4 responses after repetitive immunization with messenger RNA-based COVID-19 vaccines. Int J Infect Dis 2023;139:1–5. DOI: 10.1016/j.ijid.2023.11.028.
Routhu NK, Stampfer SD, Lai L, et al. Efficacy of mRNA-1273 and Novavax ancestral or BA.1 spike booster vaccines against SARS-CoV-2 BA.5 infection in non-human primates. Sci Immunol 2023:eadg7015. DOI: 10.1126/sciimmunol.adg7015.
Buhre JS, Pongracz T, Kunsting I, et al. mRNA vaccines against SARS-CoV-2 induce comparably low long-term IgG Fc galactosylation and sialylation levels but increasing long-term IgG4 responses compared to an adenovirus-based vaccine. Front Immunol 2022;13:1020844. DOI: 10.3389/fimmu.2022.1020844.
Uversky VN, Redwan EM, Makis W, Rubio-Casillas A. IgG4 Antibodies Induced by Repeated Vaccination May Generate Immune Tolerance to the SARS-CoV-2 Spike Protein. Vaccines (Basel) 2023;11(5). DOI: 10.3390/vaccines11050991.
In this article by Patterson et al [Patterson BK, Francisco EB, Yogendra R, et al. Persistence of SARS CoV-2 S1 protein in CD16+ monocytes in post-acute sequelae of COVID-19 (PASC) up to 15 months post-infection. Front Immunol. 2022 Jan 10;12:746021. doi: 10.3389/fimmu.2021.746021.], it might be possible that integration occurred in this individual. Whether it was due to shedding or not remains to be determined.
For patients with IgG spike antibody titres at or above a dilution of 1/25,000 (BTW is this IgG1/3 or IgG2/4? and does it matter?), this might be an indication of integration of the vaccine derived nucleotide sequences into genomic DNA (i.e., the dreaded genetic modification of humans). Instead of trying to biopsy each organ in the body, we could purify genomic DNA from plasma. The contents of recently lysed cells (say the ones expressing the vaccine sequence for spike which are killed by the immune system in the presence of ivermectin and zinc) could be examined for gene copy number for the spike gene and for HERV-K102 [see my real time PCR method used in Laderoute MP et al, Open AIDS Journal, 2015 on how to run the tests for genomic DNA and exclude cDNA of the HERV-K102 particles. If HERV-K102 copy number is elevated (for example in people with high levels of spike antibody and not in those with little or no antibody and there is no active SARS-CoV-2 infection, this might imply that the exosomes associated with shedding might be the 100 nm HERV-K102 particles. In this case, one would like to also examine genomic DNA in macrophages/monocytes and in the bone marrow progenitors of the monocytes/macrophages. It is possible that integration might more commonly occur as a direct consequence of shedding (from HERV-K102 particles produced in sebocytes found in sebaceous glands in the mucosa carrying the RNA or DNA sequence of spike).