


The Marvels of the HERV-K102 Virus-Anti-Virus Protection System of Humans Including Shed (Horizontal) Population Protection (and the Harms of Gene Therapy Shedding)
V.2 Evidence Consistent with Protective Shedding from those Vaccinated with Only One Dose While for Two Doses Shedding Putatively Promotes DEATH in the Unvaccinated (Updated April 11, 2024).

In the previous substack article on February 23, 2024, the notion of shedding by the vaccinated contributing to deaths in the unvaccinated was examined.
__________________________________________________________________
Attempts to Quantify Impact of Shedding in the Unvaccinated and Vaccinated (UK ONS Data, 2021 & 2022)

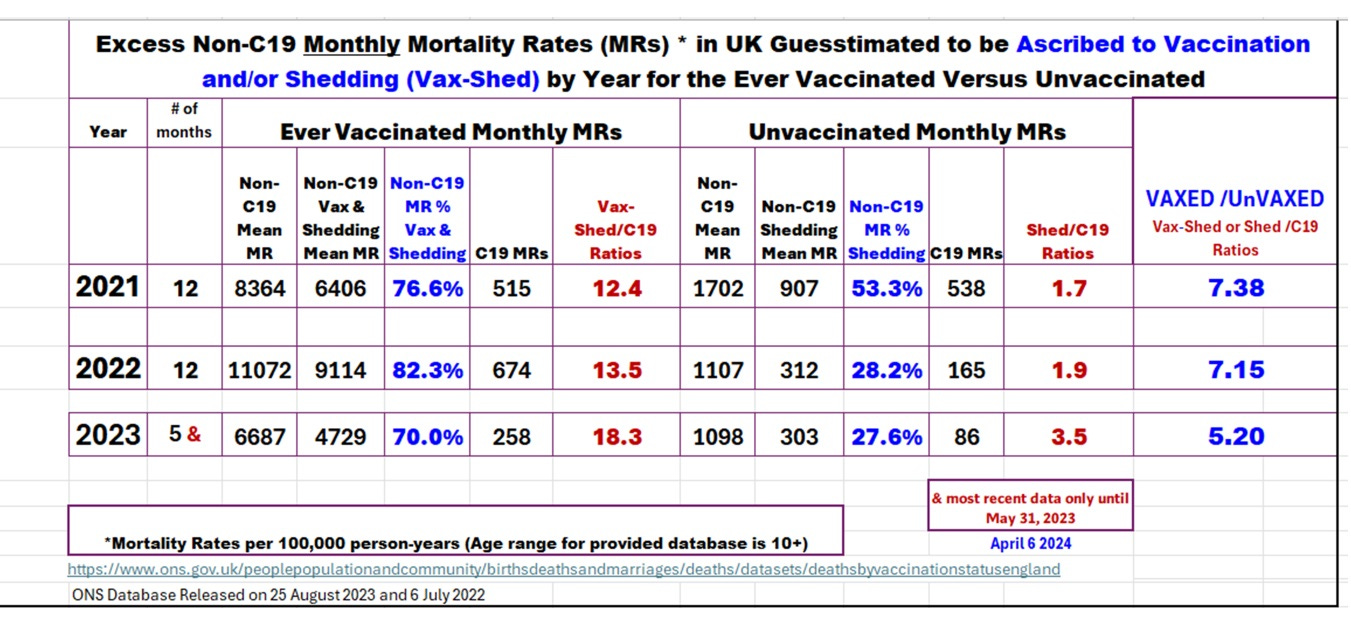
Image 1. UK Non-COVID-19 (non-C19) and COVID-19 (c19) Mortality Rates (per 100,000 person-years) by Vaccination Status for 2021 and 2022 DATA FROM: Jan 2021 to May 2022 from ONS released July 6, 2022 https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/deaths/bulletins/deathsinvolvingcovid19byvaccinationstatusengland/deathsoccu…
____________________________________
Recall that in the comparison of the non-C19 over the C19 mortality ratios, these peaked in the unvaccinated whenever the peaks occurred in the vaccinated. These peaks related to recent vaccination in the vaccinated (around when 45% of the 65 to 75 years of age were vaccinated). This suggested shedding from the vaccinated to the unvaccinated, where shedding also caused death in the unvaccinated (IMAGE 1 & 2 yellow highlights). The highest risk of mortality pertained to the second dose when IgG1/3 spike antibodies were formed.
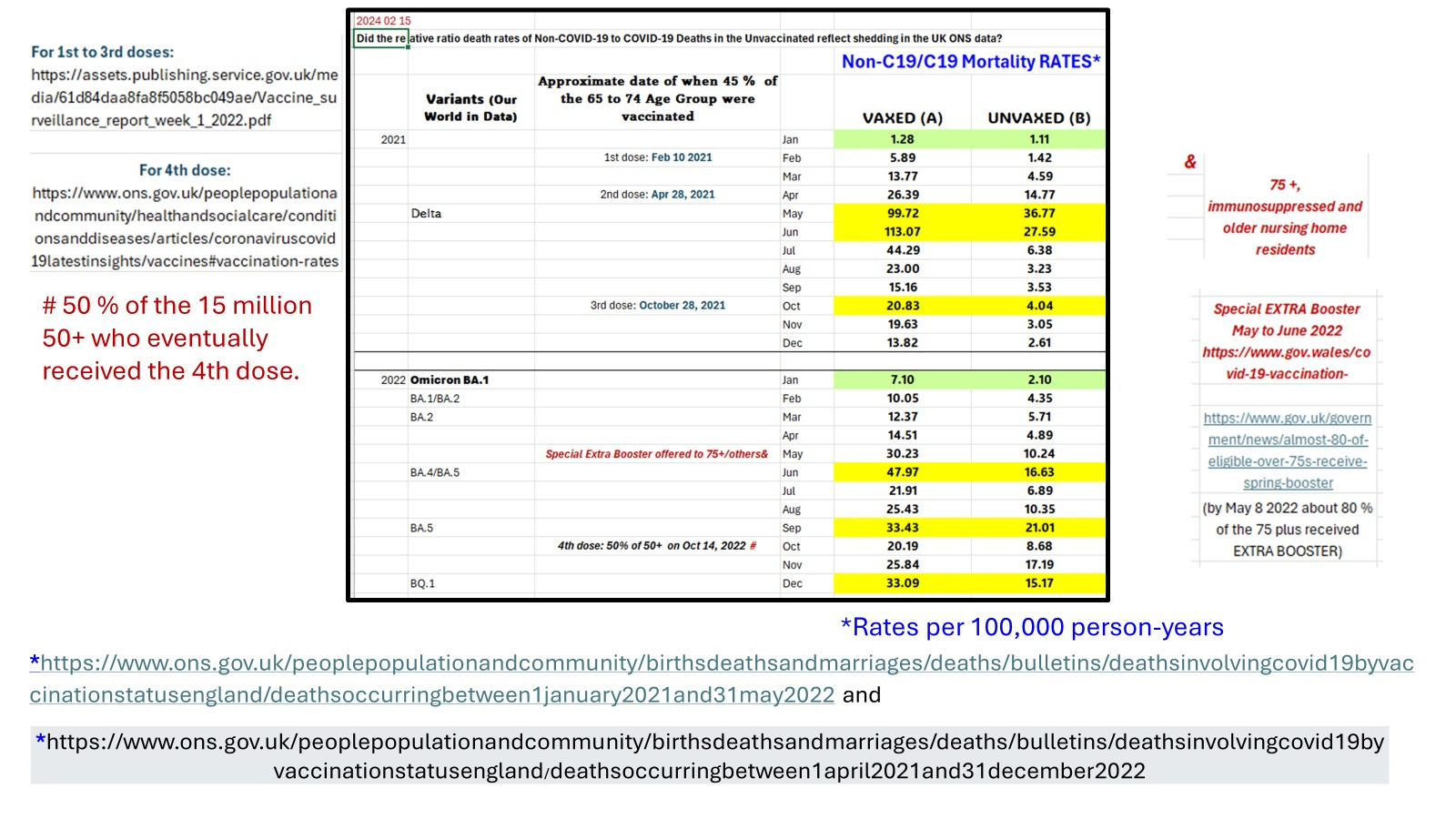
IMAGE 1. Peaks and Troughs in the Unvaxed Mirror that in the Vaxed for Non-C19/C19 Mortality Rates
It should also be noted that there were two nadirs highlighted in green; one with the initial first dose in January 2021 and one when omicron fully emerged in January 2022 (IMAGE 1 & 2 green highlights). These months correlated with periods of negative excess all-cause mortality (see Our World in DATA) and is thought to be due to heterologous protection promoted by the activation of trained INNATE immunity in foamy macrophages [1].
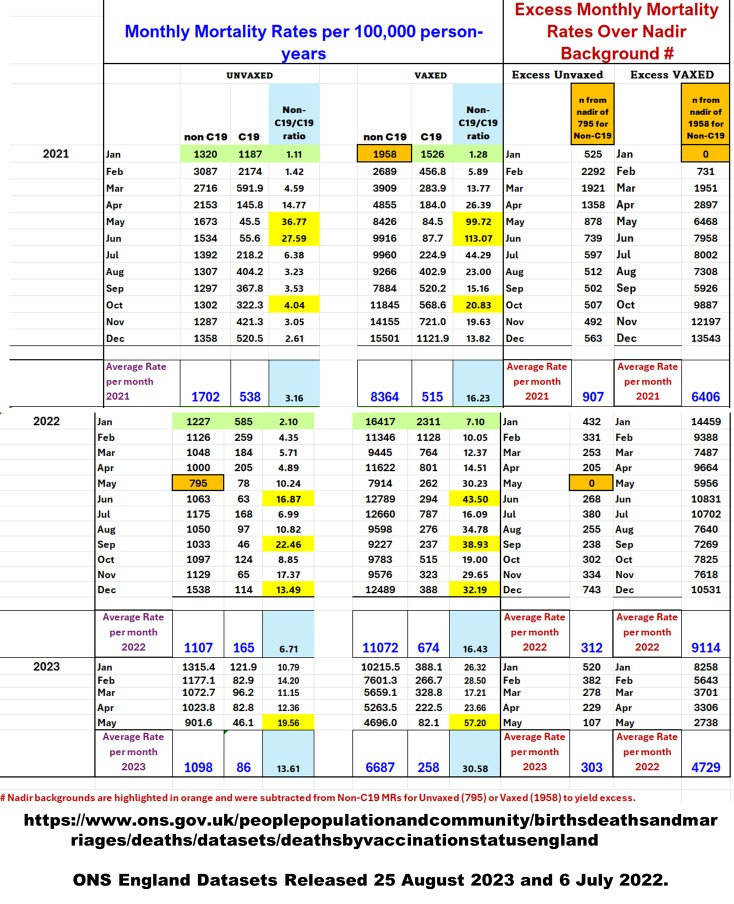
IMAGE 2. Guesstimates for Lethal Vaccine & Shedding Adverse Events Subtracts the Lowest Non-C19 Monthly Mortality Rate Observed Over 2021 and 2022 (795 for the Unvaxed and 1958 for the Vaxed)
Note that the guesstimates of the rates of death related to shedding indicate that in the unvaccinated the shedding may have killed more patients than SARS-CoV-2.
For the vaccinated, vaccination combined with shedding may have also SIGNIFICANTLY killed more patients than SARS-CoV-2.
Overall the guesstimates indicate the mRNA gene therapy shots killed more patients than SARS-CoV-2 surprisingly, including the unvaccinated!
We now know the critical INNATE protection involves HERV-K102 particle production in foamy macrophages (IMAGE 3) and involves the release of the particles by lysis [1]. This launches the HERV-K102 protector system which includes antibodies to HERV-K102 envelope and gamma delta T cells both which recognize HERV-K102 envelope on virally transformed cells [1]. Remarkably, because RNA pandemic viruses like HIV-1 and SARS-CoV-2 are enveloped viruses this means their virions also carry the HERV-K102 envelope protein. So the antibodies to HERV-K102 envelope are also neutralizing antibodies and would clear SARS-CoV-2 virions [1]!
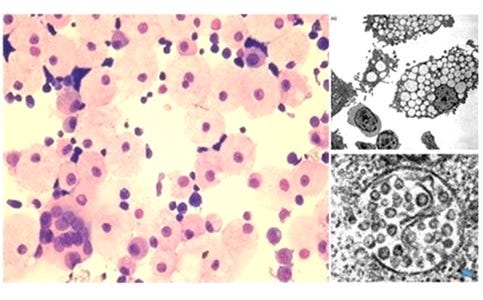
IMAGE 3. Foamy macrophages producing high levels of HERV-K102 particles.
The question arises as to why SHOULD the shed vaccinal spike mRNA/cDNA be so deadly in the unvaccinated.
As illustrated in IMAGE 4, the lipid nanoparticles entering the sebocytes (specialized macrophages constitutively producing HERV-K102 particles [1]) in the mucosa of the upper respiratory tract (URT) of the newly vaccinated, are proposed to hitch a ride with the HERV-K102 particles that have functional reverse transcriptase and integrase [1]. When spike IgG1/3 are produced in the URT such as after the second dose, this targets the LNPs to macrophages so with the second dose more of the sebocytes are proposed to be contaminated than the first dose (see IMAGE 5). So shedding involving the HERV-K102 particles following the first dose is generally protective, while shedding after the second dose is more likely to be contaminated with spike mRNA and cDNA and not protective. When the gene therapy payload is delivered to the host in this manner instead of the LNP direct delivery (which lacks reverse transcriptase and integrase), there is a much higher likelihood that spike mRNA/cDNA would be integrated in the DNA in the new host which could then pump out more copies of spike protein.
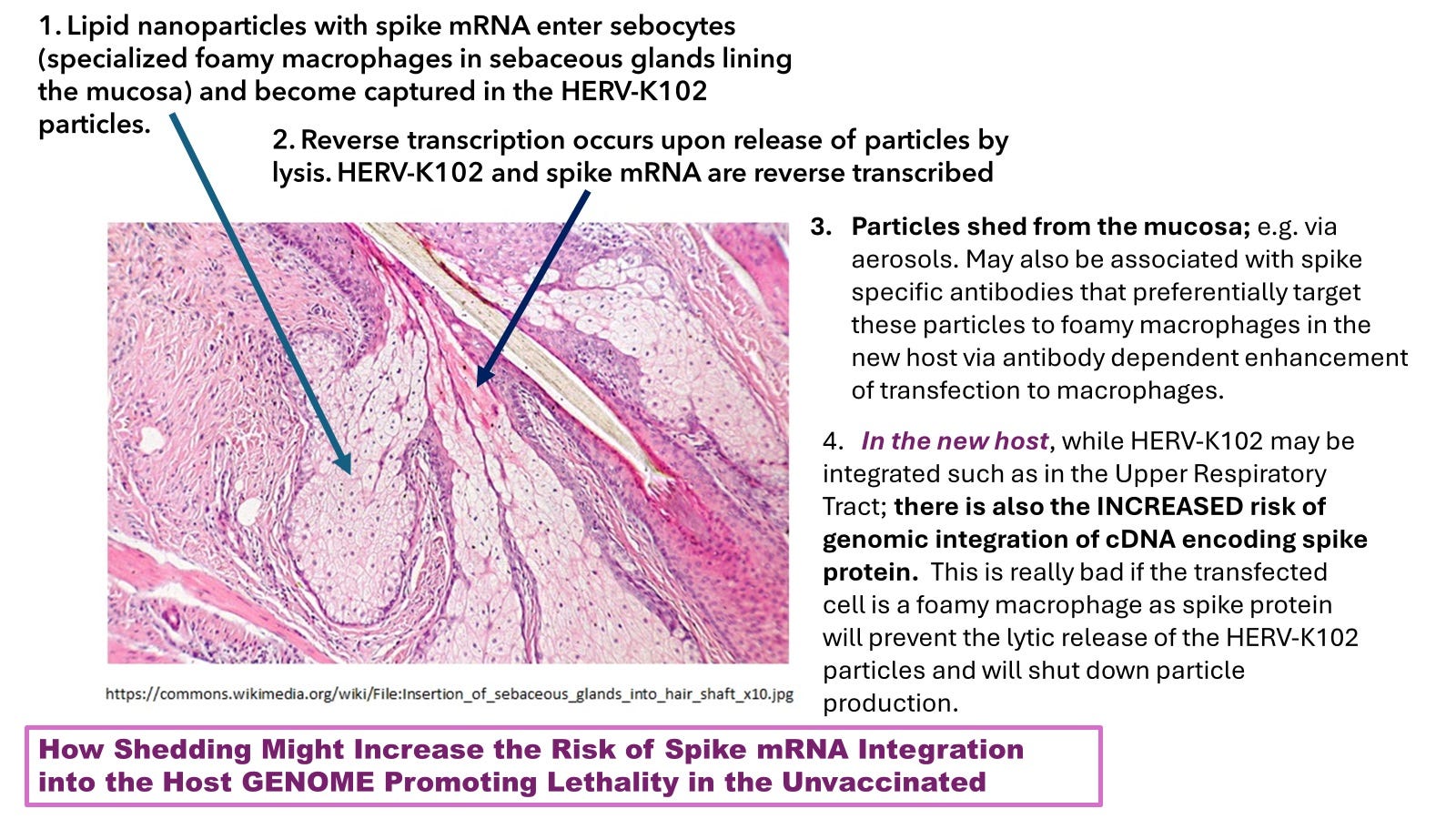
IMAGE 4. Sebocytes in the mucosa are specialized lipid-body negative foamy macrophages (M1 like) that constitutively produce HERV-K102 particles and release them by lysis as sebum.
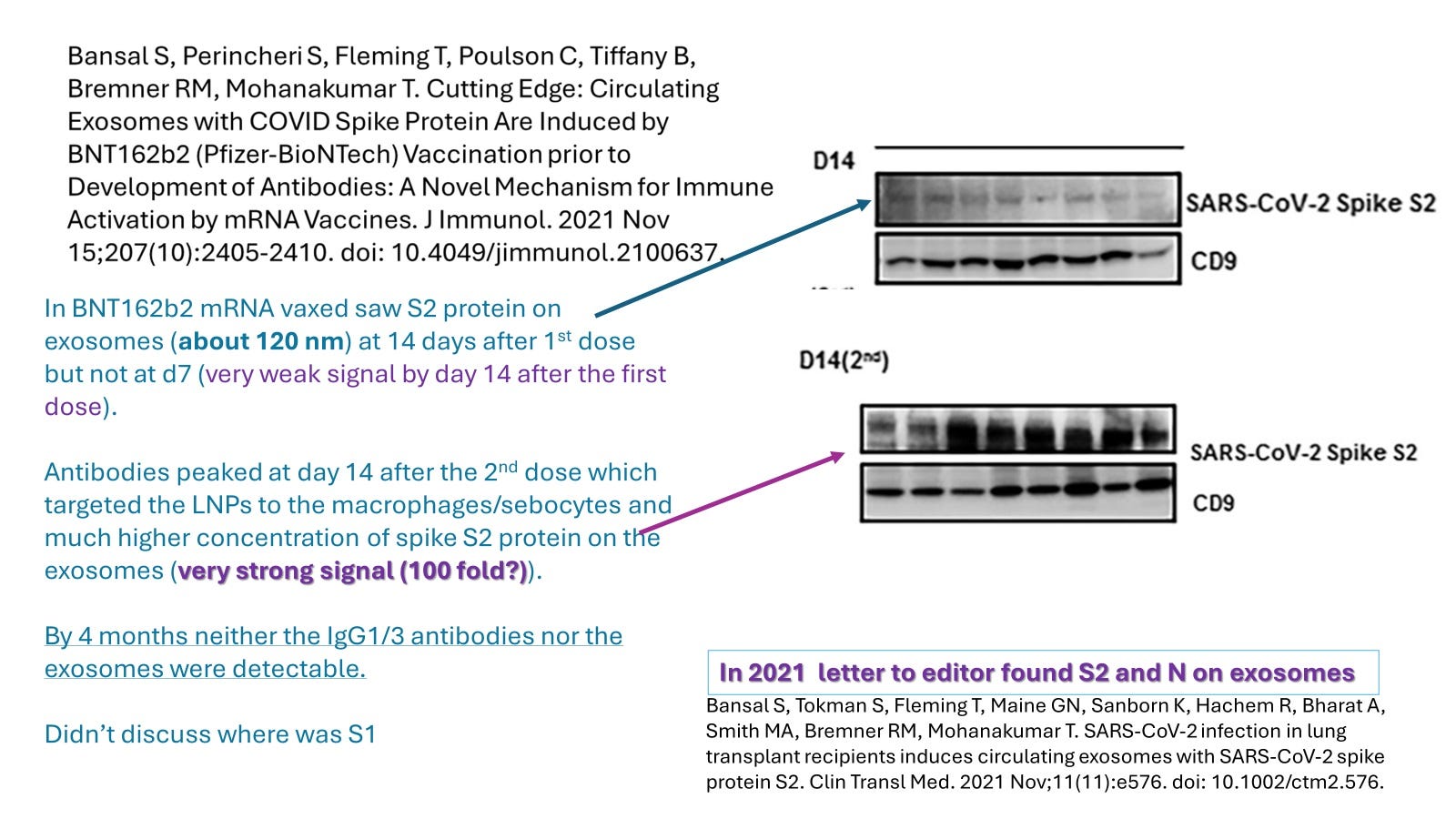
Image 5. In Pfizer-BioNTech mRNA vaccinated vaccinees the amount of spike protein detected on/in the 120 nm exosomes (presumed HERV-K102 particles) in plasma increases significantly when the IgG1/3 spike antibodies are induced showing that these antibodies trigger targeting of the LNP to the macrophages by antibody dependent enhancement (ADE) of entry into macrophages which results in the contamination of the HERV-K102 particles converting them from protector to pathogenic!
NB: The CD9 antigen shown represents the main tetraspanin of the macrophage-derived exosomes and controls for levels of exosome extracts run on the gel. Also these authors detected only S2 on the plasma exosomes implying S1 was cleaved and shed directly into the plasma. Finally, they indicated that the spike IgG1/3 antibodies disappeared by 4 months potentially consistent with their conversion to IgG4. Also at this time, the HERV-K102 particles are no longer produced. It is not clear if this significantly drops by around 3 months or about 120 days.
Note the same would happen in the URT with the infestation of sebocytes with the LNP spike mRNA/cDNA except here the contaminated exosomes are shed horizontally to third parties. This raises major ethical, practical and medical issues including constitutional rights, political correctness, public health fiascos, insurance issues, and criminal manslaughter issues, as well as whether the newly mRNA vaccinated should be isolated for 3-4 months, and so on.
That there are protector exosomes such as from patients with mild COVID-19 and harmful exosomes such as from patients with severe COVID-19 has been published [Pesce E et al., Frontiers in Immunology January 2022].
To follow the rest of the arguments, one has to understand that 1) in the unvaccinated there is little or no spike IgG in the URT but the mRNA vaccines induce lots and 2) there does not seem to be much conversion of the spike IgG1/3 in the URT to IgG4 in the vaccinated if we believe the Cleveland Clinic data which shows the infection rates for SARS-COV-2 symptomatic infection increase proportional to dose number (reviewed in [1]). Therefore with each mRNA vaccination more and more of the HERV-K102 particles from sebocytes are contaminated with spike protein (and the spike mRNA/cDNA).
So the unvaccinated only shed protective HERV-K102 particles while the vaccinated shed Pathogenic Exosomes (the mix of pathogenic to protective exosomes being related to the levels of spike IgG1/3 which go up in the URT with each dose of the mRNA vaccine.) This shedding risk apparently persists for up to 3-4 months [Bansal S et al., 2021, and Image 5].
As discussed elsewhere there are two types of ADE in COVID-19, one in the URT and one in the lungs (LRT) [1]. The ADE in the URT involves IgG1/3 binding to FCGR2A (classical ADE) and where basigin (BSG/CD147) and FCGR2B are downregulated on the activated sebocytes and thus, not applicable [2]. FCGR2B is the FC receptor mediating the inhibition of macrophage activation which is triggered by “IgG4 in the presence of spike protein”. But as best as I can tell the IgG1/3 in the URT do not switch to IgG4.
In contrast, in severe COVID-19 as measured in the bronchoalveolar lavage fluids (BALF), there is a novel type of ADE where presumably the affinity maturated (high affinity) IgG now of the IgG4 isoform, inhibits the spike:ACE2 binding allowing spike protein to preferentially bind BSG and thus target the cells of the immune system especially the macrophages [3]. It is thought triggering BSG generates a strong inflammatory signal associated with cytokine storm while other evidence suggests SARS-CoV-2 during the conversion of the M1-like protector foamy macrophages to the M2-like pathogenic macrophages also imparts the proinflammatory signal involving deregulated NFKB1 (Image 6).
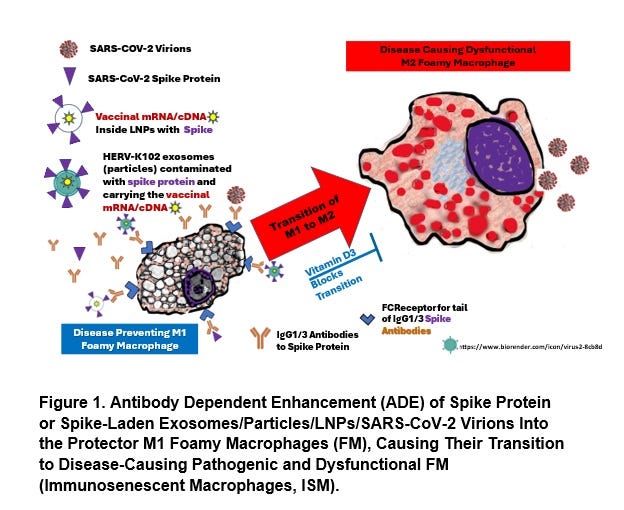
IMAGE 6. Conversion by SARS-CoV-2 of the Protector Lipid Body Negative Foamy Macrophages to Pathogenic Lipid Body Positive Foamy Macrophages (& Might be Blocked by Optimal Vitamin D3) [1].
If the IgG1/3 antibodies in the URT are shed with the contaminated and now pathogenic HERV-K102 particles, this would target the macrophages in the new host (including the unvaccinated) and knock out host innate immunity increasing mortality. Unfortunately there is evidence for aerosol transfer of spike IgG antibodies caught by masks [Ross M. Kedl, Elena W. Y. Hsieh, Thomas E. Morrison, Gabriela Samayoa-Reyes, Siobhan Flaherty, Conner L. Jackson, Rosemary Rochford; Evidence for Aerosol Transfer of SARS-CoV-2–Specific Humoral Immunity. Immunohorizons 1 May 2023; 7 (5): 307–309. https://doi.org/10.4049/immunohorizons.2300027].
This greatly increases the risk of death and includes immunosenescence effects which induces cardiovascular disease, cancers, and other infections. However it is also the persistent expression of spike protein which is extremely toxic, that could cause death directly and even suddenly.
If we look at changes in the mortality rates (C19 versus non-C19) within the month of the admininstration of the mRNA dose (IMAGE 7), we see that:
The first dose in the vaccinated (A) generates protection (presumed shedding of clean HERV-K102 particles to the unvaccinated) against C19 mortality and less so non-C19 mortality. Due to the toxicity of the mRNA gene therapy shots, the vaccinated show a 24 % increase in non-C19 mortality.
The second dose (B) generates high levels of C19 death in the vaccinated (promotes ADE mediated COVID-19 progression and death [1]) but also to the unvaccinated as the ADE spike antibodies target the contaminated HERV-K102 particles to macrophages knocking out critical host defenses and allows for high levels of spike expression.
The third dose (C) which generates the conversion of spike IgG1/3 (ADE promoting) to IgG4 (blocks ability to activate macrophages but no longer promotes immunosenescence which causes non-C19 mortality) associated with a lower increase in C19 mortality in the vaccinated. However the Cleveland Clinic Data argues that this conversion does not occur in the upper respiratory tract (URT). Therefore the spike antibodies are IgG1/3 in the URT, and again target the contaminated HERV-K102 particles to the macrophages in the unvaccinated. In C, the level of shed HERV-K102 generated heterologous protection against non-C19 mortality has diminished from -22% (A), -10% (B) and is now -1% (C).
For the fourth dose involving only the 75 + and high risk individuals, about 80% had received this extra booster by May 2022 when Omicron BA.2 was circulating. Possibly because the spike protein of Omicron was so different from the original Wuhan variant of the vaccines, we see in E that across the board for both vaccinated and unvaccinated, Omicron infection reduces all-cause mortality (plus Omicron did not produce the lower respiratory track pathology involving pneumonia). So for D we see slightly less decreases in C19 mortality rates (for the vaxed and unvaxed) but because in the URT, the spike antibodies are still IgG1/3, the shed contaminated particles target the macrophages via ADE and the non-C19 mortality shows an increase for the unvaccinated (D).
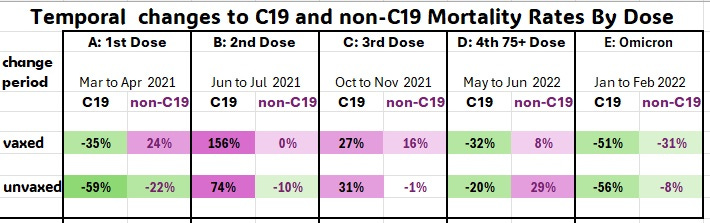
IMAGE 7. Data (extracted from Image 2) consistent with the notion that shed HERV-K102 particles can provide protection to the unvaccinated (C19 and non-C19) while those contaminated with spike mRNA/cDNA and which target macrophages in the new host via spike IgG1/3 promote host demise.
Beneficial reduction of mortality rates shown in green while adverse increases in mortality are shown in maroon. The change period examined allows for 2 weeks for the change and another 10 days to affect mortality and represents the midpoint of when about half of the 65 to 75 years of age group would have received that dose.
Note for D only the 75+ were vaccinated and those at very high risk.
Note that each time the Pfizer-BioNtech mRNA is injected into the vaccinated there is generally an induction of non-C19 death consistent with its toxicity. However, exposure to the omicron variant in January 2022 (E) diminished both C19 and non-C19 mortality in both the vaxed and unvaxed probably because it naturally induced innate immunity and heterologous protection.
In D note the higher % level increase in non-C19 mortality (D) for the unvaxed (29%) over the vaxed (8%) which is yet to be explained although it could be simply because the April to May mortality rates for the vaxed were already high (Image 2).
Overall, Image 7 shows when spike IgG1/3 is absent (A and/or E) in the shedder, there is a net benefit of the shed (uncontaminated = no spike protein or spike mRNA/cDNA) HERV-K102 particles from the vaccinated on all-cause mortality in the unvaccinated. However, once the vaccinated develop IgG1/3 to spike following the second dose, we see a massive increase in C19 mortality in both the vaxed and unvaxed which probably relates to antibody dependent enhancement (ADE) of infection of the contaminated shed particles to macrophages in the new host.
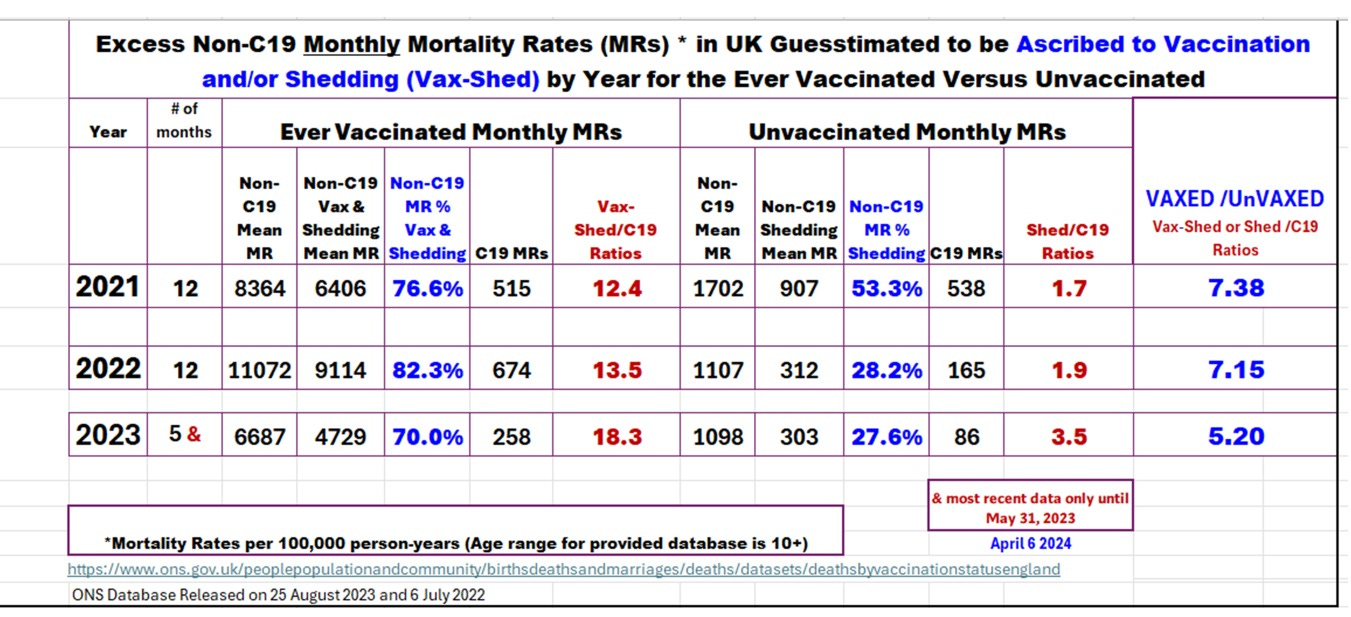
IMAGE 8. Guesstimates of Impacts of Vaccination—Shedding in England on Non-C19 mortality from 2021 to 2023 in Comparison to the Unvaccinated (largely the Pfizer-BioNTech mRNA gene therapy shots).
In Image 8, for the unvaxed there are apparently more deaths guesstimated to be due to shedding than due to SARS-CoV-2 infection (COVID-19 mortality).
{NB: Shedding would also increase the risks of COVID-19 deaths but which are too difficult to estimate, so the risks of shedding related deaths compared to C19 deaths are most certainly underestimated in Image 8.}
There may be three good reasons for why shedding of the gene therapy product is more dangerous than the mRNA vaccines themselves or SARS-CoV-2 infection:
There may be a much higher (many log increased) risk of integration when the SARS-CoV-2 mRNA/cDNA hitch-hikes a ride with the protector HERV-K102 particles because they reverse transcribe upon exit (i.e., lytic release from the sebocytes) and also contain functional integrase as shown in Image 9 below; accordingly, shedding may have a higher risk of mortality than vaccination or SARS-CoV-2 infection due to this increased risk of integration;
For the unvaccinated, in the upper respiratory tract (URT), even though the mRNA unvaccinated do not have spike specific IgG1/3 in the URT, the contaminated HERV-K102 particles are coming in with spike specific IgG1/3 which targets the exosomes to sebocytes in the URT; or particularly with deep breaths associated with strenuous exercise especially indoors, direct enhancement of infection of macrophages in the lower respiratory tract (LRT) is likely; this causes “micro-clotting” of the small capillaries in the lungs, meaning there may be direct inoculation of the circulation with the pathogenic exosomes which may carry an increased risk of myocarditis/pericarditis (etc). Interestingly, recent evidence suggests the spike containing exosomes in plasma of patients with Post-Acute Sequelae of COVID-19 (PASC) correlate with D-dimer levels and not CRP nor BMI [Craddock V et al., J Med Virol, Feb 2023]. Potentially this implies the pathogenic exosomes may be directly causing myocarditis and other heart issues. Indeed, others have reported that despite many PASC patients exhibiting hypertension and/or other cardiovascular issues, the risk of PASC does NOT correlate with hypertension nor with any cardiac problem [Sneller M et al., Ann Intern Med, 2022], possibly because many of these patients who were shed upon and who may have developed myocarditis, did not live long enough to be included in the PASC category. Thus, the risk of myocarditis and death in the unvaccinated would be much higher than SARS-CoV-2 (see UK data in Image 8 for higher risk of death due to shedding than SARS-CoV-2).
For the mRNA vaccinated, essentially the spike specific IgG1/3 in the LRT/blood remain for up to 4 months then get converted to IgG4, the so-called tolerogenic antibodies and this conversion is expedited by the third dose [Irrgang P et al., Sci Immunol Jan 2023]. In contrast the spike IgG1/3 in the URT remain and get boosted with each shot. For example the risk of SARS-CoV-2 infection goes up with each subsequent mRNA dose according to the Cleveland Clinic DATA (Image 10). However, people who were infected prior to the two doses of the mRNA do NOT convert the spike IgG1/3 to IgG4 (no matter how many doses) [Kiszel P et al., Sci Reports Aug 2023; Akhtar M et al., Frontiers in Immunol, Dec 2023]. In the omicron era, there does not seem to be as much lung pathology (ie., pneumonia) as the pre-omicron variants possibly because the spike protein is so different from the delta variant and might not have affinity for BSG and/or by the time many vaccinated people were infected with omicron in December 2020 to January 2022, the prevailing spike antibody isotypes were the IgG2/IgG4. This means in the 3rd and 4th quarters of 2021, in the USA much of the excess mortality related to residual spike IgG1/3 in the lungs or blood. According to Image 11, this appears to suggest the risk of SARS-CoV-2 infection prior to the 2 doses of mRNA vaccine was because the younger one was, the more likely that an infection occurred prior to mRNA COVID-19 vaccination. Thus the younger were at proportionately higher risk because it was less likely their IgG1/3 would class switch to IgG4. So for the mRNA vaccinated, when compared with the unvaccinated, the shedding and the COVID-19 deaths are elevated over the unvaccinated for the UK (Image 8). As well the risk of shedding induced death in the vaccinated exceeds the non-C19 and the C19 deaths and this risk is maintained into 2023. However for the unvaccinated the shedding proportion diminished from 53 % in 2021 to about 25 % in 2022 and part of 2023.
Overall, the UK population data in Image 8, strongly suggests that shedding is a more lethal exposure in those who received 2 doses of the mRNA vaccine than by SARS-CoV-2 or due to the direct toxicity of the mRNA vaccines. Unfortunately this data in Images 7 and 8 also shows shedding was lethal to the unvaccinated.
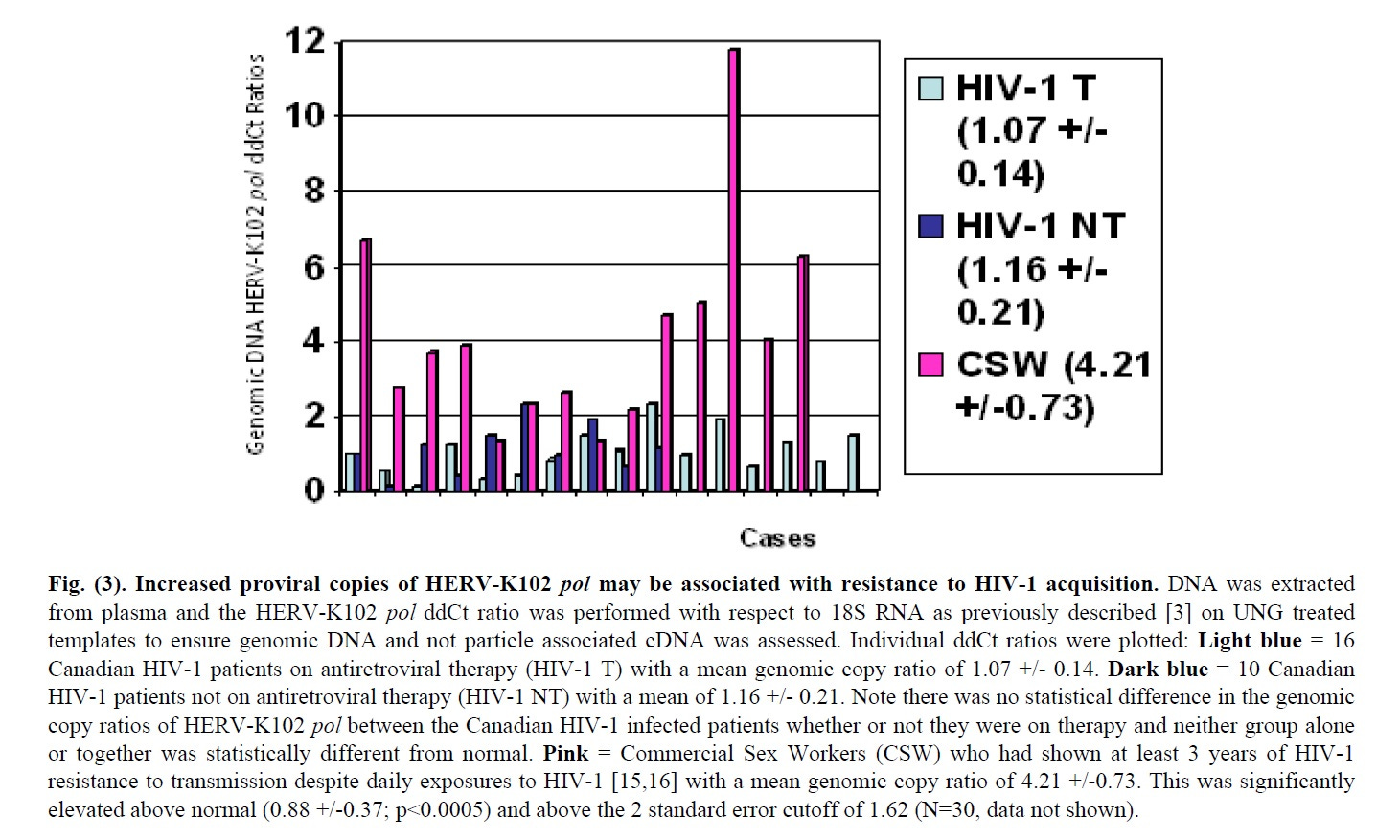
IMAGE 9. Evidence that HERV-K102 particles contain functional reverse transcriptase and integrase.
This novel virus anti-virus protection system undergoes amplification via retroviral reverse transcription and integration into host DNA genome, and this potency (increased proviral copy number) has been linked to resistance to HIV-1 acquisition (IMAGE 8) where HIV-1 is another pandemic, enveloped RNA virus [reviewed in ref. 1].
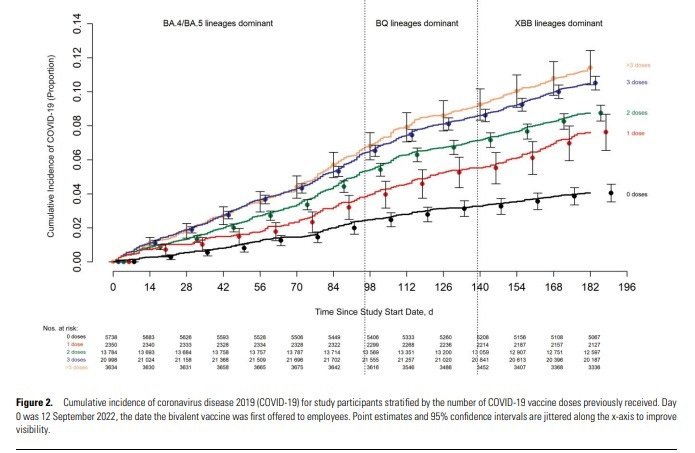
Image 10. The Cleveland Clinic Symptomatic Infection DATA.
From: Shrestha NK, Burke PC, Nowacki AS, Simon JF, Hagen A, Gordon SM. Effectiveness of the coronavirus disease 2019 bivalent vaccine. Open Forum Infect Dis. 2023 Apr 19;10(6):ofad209. doi: 10.1093/ofid/ofad209.
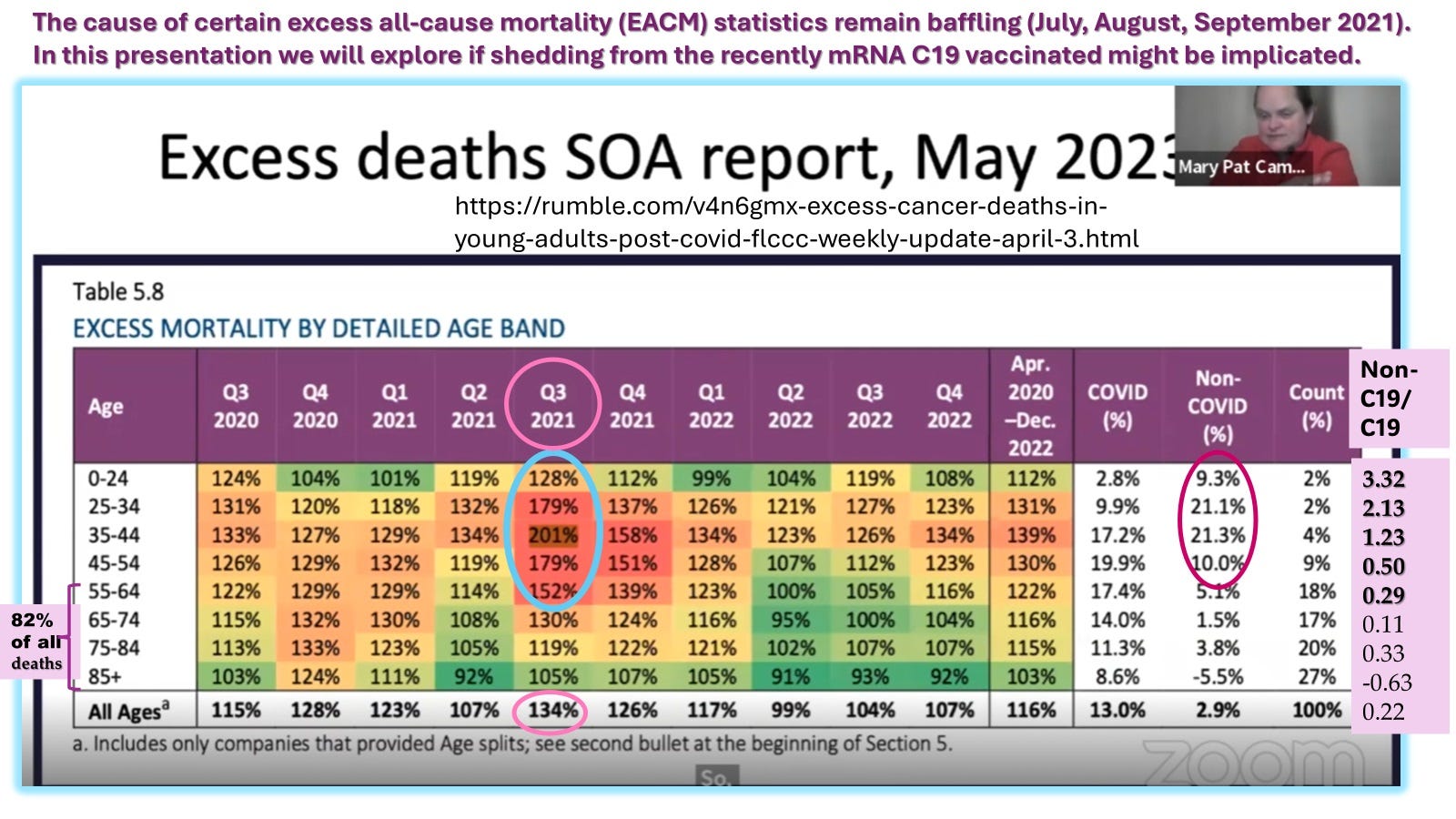
Image 11. Relative (% increase in proportions not the count) excess of all-cause mortality in the 3rd and 4th quarters of 2021 in the USA tended to focus on the under 40/50. Indeed the risk of non-C19 to C19 death ratios for the period April 2020 to December 2022 revealed the younger one was, the more likely the excess risk percentage over 2019 for that age group.
It is alleged that the HERV-K102 INNATE protection system of foamy macrophages is so potent, that it may account for human survival over other extinct hominins, at least in part [see discussion in ref 1]. Remarkably in part this may be due to horizontal transfer of trained innate immunity (Image 7: A and E) via shed HERV-K102 particles (not contaminated with gene therapy spike protein). This prepares the new host with a pre-launched HERV-K102 system (which may argue against the use of masks during a pandemic provided no gene therapy vaccines are used).
However, it is known that gene therapy leads to shedding of the new genes to third parties which is why the FDA requires shedding and integration studies of all gene therapy products.
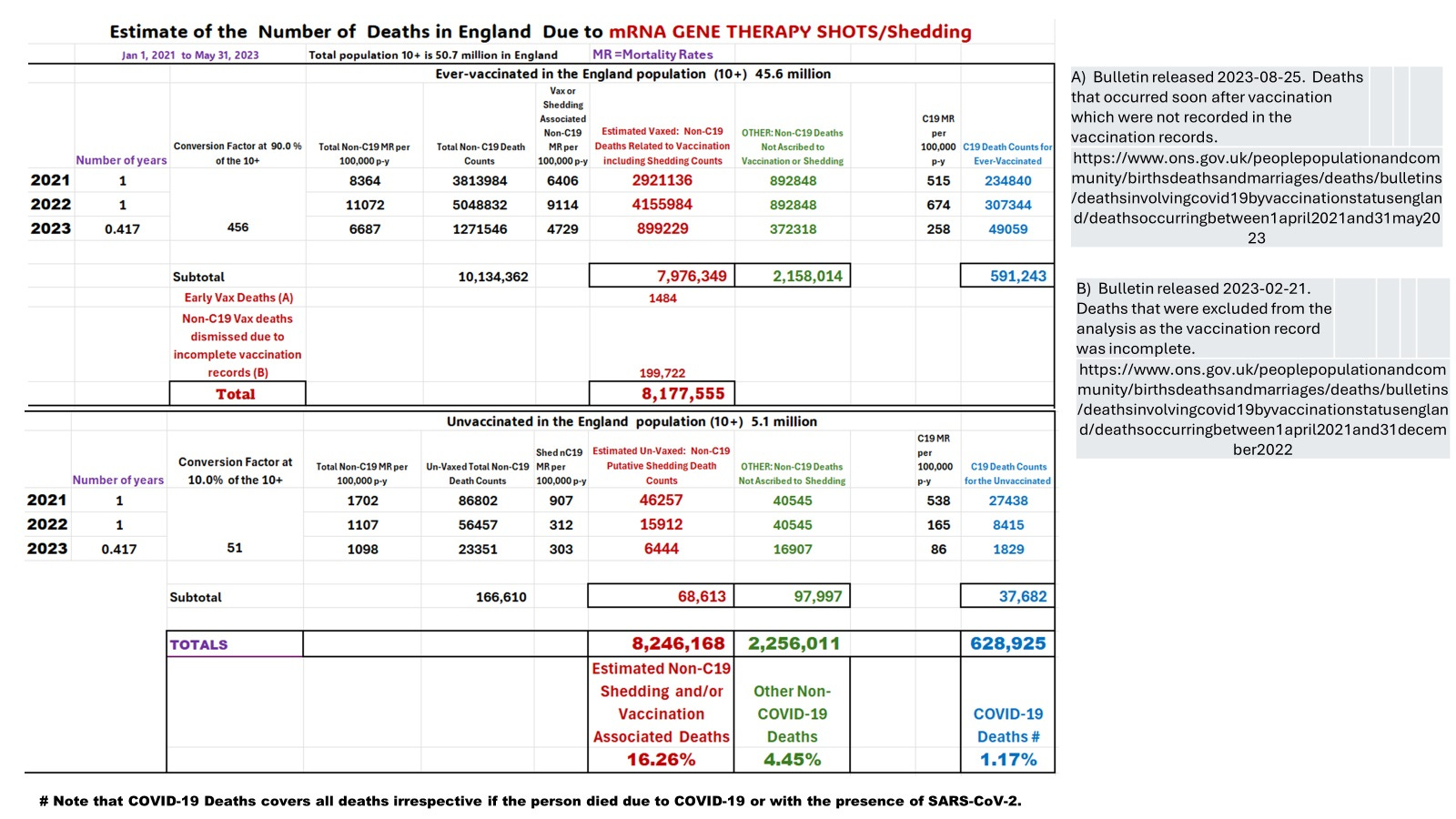
Image 12. The potential impact of mRNA gene therapy product lethal adverse events including SHEDDING on the level of all-cause mortality MAY HAVE BEEN severely underestimated and thus largely unappreciated.
It seems a lot of resources were spent on the counternarrative when health officials suddenly realized that the rates of all-cause mortality were skyrocketing especially in the younger adults. This is when Fisman published his contrived modeling paper in the CMAJ (April 25, 2022) saying the unvaccinated should have been locked up and the keys thrown away at least according to Dr. R.N. Watteel’s book called “Fisman’s Fraud”.
In fact, it was the person who received the second or more mRNA gene therapy products who should have been locked up (according to the data in Image 12). They were walking time bombs, silently killing the folks around them. But the folks didn’t know, and besides stealth, it frequently involved sudden death. You didn’t know until it was already too late.
The vast majority of victims tended to be the younger adults because they were more likely to have caught SARS-CoV-2 infection before receiving two doses of the mRNA gene therapy shots (administration was the eldest first and then in descending order with the youngest last) and thus, had more of the deadly spike-specific IgG1/3 remaining after two doses of the mRNA vaccines.
GOOD NEWS:
For the first time ever, evidence is presented consistent with the notion that protector HERV-K102 particles released from the URT mucosa at higher levels upon innate immune activation by one dose of the mRNA vaccines, (and presumably also during natural infections such as Omicron in January 2022), provides horizontal protection against all-cause mortality in the yet uninfected host. Aside from the known vertical transmission of immunity during pregnancy and breast-feeding, this is the first instance of protection of the yet uninfected by the putative horizontal pre-activation of HERV-K102 in the new host.
BAD NEWS:
The gene therapy mRNA/cDNA COVID-19 vaccines allegedly have unleashed a very deadly mechanism involving shedding for culling the human population including those who never directly received the shots (the unvaccinated). Most of the shedding precipitated deaths may relate to myocarditis and similar types of cardiovascular deaths. According to the CDC Wonder VAERS database perhaps about 25 % of these myocarditis deaths could involve sudden death (within 24 hours).
In conclusion, all gene therapy shots especially those administered to healthy people under the guise of ‘safe and effective vaccines’ should be immediately banned including their study in clinical trials due to the existential threat to the survival of the Homo sapiens species uncovered here.
The mRNA/cDNA gene therapy shots are BIO-WEAPONS and must be banned!
mRNA gene therapy vaccine is an oxymoron.
REFERENCES:
Laderoute, M. Antibody Dependent Enhancement (ADE) of Infection into Macrophages Validates the Importance of HERV-K102 Particle Production for Pandemic Preparedness. Preprints 2023, 2023120185. https://doi.org/10.20944/preprints202312.0185.v1.
Ziegler CGK, Miao VN, Owings AH, et al. Impaired local intrinsic immunity to SARS-CoV-2 infection in severe COVID-19. Cell. 2021 Sep 2;184(18):4713-4733.e22. doi: 10.1016/j.cell.2021.07.023.
Ren X, Wen W, Fan X, et al. COVID-19 immune features revealed by a large-scale single-cell transcriptome atlas. Cell. 2021 Apr 1;184(7):1895-1913.e19. doi: 10.1016/j.cell.2021.01.053.
Please see new comment posted on X https://twitter.com/hervk102/status/1770827757674537343 on March 21, 2024 concerning differential impact of shedding on the unvaxed (no spike specific IgG4) versus the vaxed (with high levels of IgG4) and how vitamin D3 greater than 50 ng/ml can only protect those without IgG4 against all-cause mortality.
The CDC recognized long COVID in July 2021 as a new disease entity (https://www.cdc.gov/coronavirus/2019-ncov/long-term-effects/index.html?utm_source=substack&utm_medium=email) which was co-incidental with the projected maximal shedding related to increased C19 mortality (Image 5B) in the vaxed and unvaxed (for the UK population from ONS data). If morbidity is 33 times the rate of mortality, then Long COVID likely peaked around the same time. In other words, what I am saying is that Long COVID (and/or sudden death) may be moreso related to shedding from the recently vaccinated (affecting the vaxed and non-vaxed populations) and may have been particularly harmful with the emergence of the delta variant. Are the spike specific IgG1/3 from the upper respiratory tract being shed with the vaccinal spike mRNA that are captured in the exosomes (HERV-K102 particles) expressing spike at the surface which then targets the foamy macrophages in the new host (eg. sebocytes and tissue macrophages) explaining why shedding may be more dangerous with delta variant SARS-CoV-2 infection? I will summarize the exosome work in a new substack.