


Macrophage Polarization and Agents Used to Treat PASC
Making the best approach to the treatment of spike associated diseases a little more obvious. Version 4.

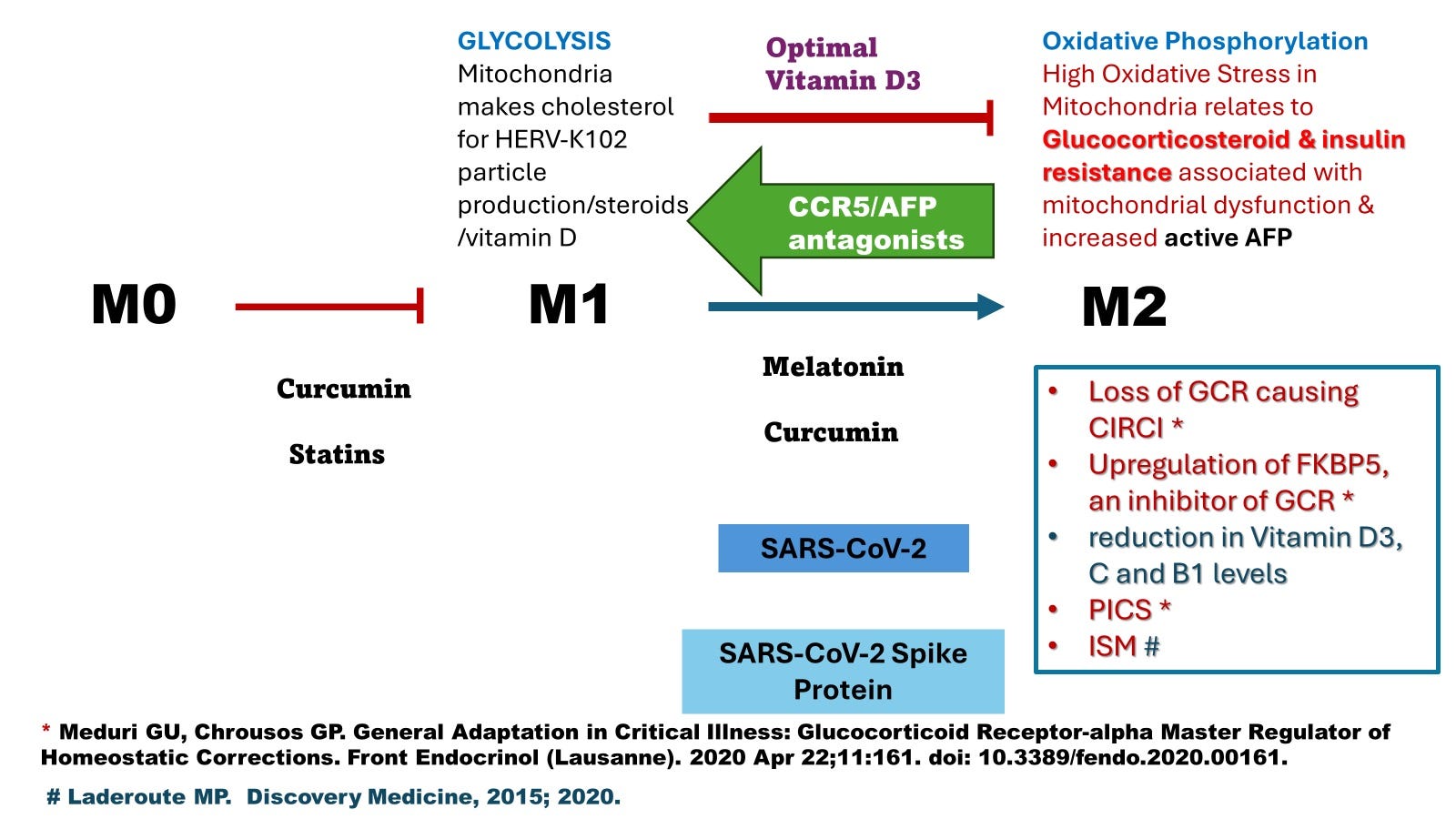
Image 1. Would favoring macrophage polarization to M2 by melatonin [1] (>2 mg per night) or curcumin [2] help in the recovery from health issues related to the presence of the toxic SARS-CoV-2 spike protein?
CIRCI =critical illness related corticosteroid insufficiency involving insufficient cortisol or corticosteroid resistance, damage to the mitochondria and dysfunction (related to oxidative stress), and a relative insufficiency of micronutrients most commonly Vitamin D3, C, and B1 (Thiamine) [3].
PICS = persistent inflammation, immunosuppression catabolism syndrome in reference to the development of a chronic critical illness (CCI) after sepsis that mimics chronic stress (elevated cortisol) and involving glucocorticoid resistance, altered hemostasis with increased risk of chronic inflammatory systemic diseases [3].
ISM =Immunosenescence of macrophages was defined as the failed lytic release of HERV-K102 particles from M1-like foamy macrophages due to depleted DHEA relative to cortisol, where DHEA binds and inactivates alpha-fetoprotein (AFP) and DHEA is lost with stress and/or aging [4,5]. ISM predisposes individuals to severe COVID-19, while SARS-CoV-2 and spike protein induce and exacerbate ISM. Signs include elevated blood pressure and CRP while symptoms are the initiation and/or progression of chronic age-associated diseases such as cardiovascular disease, obesity, tumorigenesis, cancer progression, autoimmunity, allergies, neurological diseases, etc. Reversion of ISM is by using AFP antagonists. Anti-inflammatories (that do not reverse high blood pressure or which may interfere with sleep) do not work to reverse immunosenescence of macrophages (statins, curcumin, melatonin > 2 mgs, resveratrol etc). Known AFP antagonists include DHEA (best to use 7-keto-DHEA which does not get converted to sex hormones), vitamin D3 (indirect), zinc, genistein and other isoflavones, ivermectin [6] (likely also artemisinin but this has yet to be demonstrated although it seems to have many of the biological properties of ivermectin), and anything that re-establishes p53 function (which downregulates AFP expression). AFP is “the malignancy conferring oncogene” and uses the malignancy conferring pathway of PI3K/Akt/mTOR common to Erbb2 and which NOTABLY is activated by SARS-CoV-2 and reversed by ivermectin [6].
NB. There is a significantly increased risk of S1, spike and N protein in the blood at 3 to 14 months following hospitalization over the non-hospitalized cases of COVID-19 [7].
From Image 1, is it best to let the actions of vitamin D3 (known for reducing morbidity and all-cause mortality) guide our therapy to achieve the reversion of ISM [4,5], PICS and/or CIRCI [3] ?
Image 2. Macrophages do not express ACE2, so entry by SARS-CoV-2 and spike protein relate to antibody dependent enhancement (ADE) of infection [8].
However there are two ADE mechanisms operating in COVID-19 [ attached ref [8] (page 12) ]:
1) true ADE involving FCGR2A in the upper respiratory tract (URT) with spike specific IgG1/3 [9] see illustration in Image 2, and
2) a novel type of inhibition of the spike:ACE2 interaction that switches to spike:BSG in the lower respiratory tract (LRT) [10] putatively associated with conversion of the spike IgG1/3 to IgG4 that may occur in severe COVID-19 patients.
Excerpt from reference 8 (which is attached below):
“The ADE of SARS-CoV-2 in the URT, involved classical FCGR2A expression in macrophages which were labelled as the interferon responsive macrophages []. None of the 5 types of macrophages in the URT nasopharyngeal swab samples expressed ACE2 nor TMPRSS2 indicating entry of SARS-CoV-2 into macrophages likely related to ADE. Many groups have indicated that macrophages in the lungs of severe COVID-19 patients but not those with mild or moderate disease are infected with SARS-CoV-2 where again ACE2 and/or TMPRSS2 are not expressed []. This corroborates the notion of SARS-CoV-2 entry into macrophages by ADE causing disease progression. In a very comprehensive study Ren et al [] uncovered in the lower respiratory tract (LRT), a novel type of ADE involving a switch from the ACE2: spike interaction to basigin (BSG): spike. This focused the infections on the macrophages and other immune cells and away from lung epithelial cells. In the URT, macrophages which were judged to be sebocytes (specialized lipid body negative foamy macrophages) lost expression of BSG upon their activation and as mentioned appeared to instead use the classical FCGR2A for ADE mediated entry of SARS-CoV-2 []. Thus, there are two types of ADE associated with SARS-CoV-2 infection, classical in the URT and a novel switch type in the LRT involving BSG.”
The increased PATHOLOGY of the delta variant [11] might in part relate to conversion of spike specific antibodies from IgG1/3 to IgG4 in the vaccinated. This process has been described by Dr. Geert Vanden Bossche as the steric hindrance antibodies (likely referring to IgG4) that result from steric immune refocusing [12]. These type of antibodies are quite harmful as they target SARS-CoV-2 and spike protein to macrophages (and away from epithelial cells bearing ACE2) favoring entry via BSG:spike [10]. Entry via BSG:spike in the lower respiratory tract (LRT) is more likely to result in cytokine storm [13].
According to the Cleveland Data [14] the consistent higher risk of symptomatic COVID-19 infection with each subsequent dose of the COVID-19 mRNA vaccine implies there is no conversion of the spike IgG1/3 to IgG4 in the URT meaning there is ongoing selection and transmission of variants from the URT. This process selects for more infectious/transmissible variants.
It is unlikely BSG can contribute to ADE in the URT as the activated sebocytes (specialized foamy macrophages constitutively producing and releasing HERV-K102 particles by lysis) loose expression of BSG [9]. Instead these sebocytes gain FCGR2A and loose FCGR2B with activation [9] making them very susceptible to classical ADE.
For Image 2, that Vitamin D3 blocks the transition of M1-like foamy macrophages to the Oil Red O positive Lipid body positive M2-like macrophages has been shown [15].
That SARS-COV2 and a number of pathogens cause the conversion of CD14+, CD16+ intermediate monocytes to those with lipid bodies that are M2-like (CD16+ monocytes), has been shown [16].
The M1-like monocytes/macrophages use glycolysis as their source of energy to facilitate cholesterol production while the M2-like use oxidative phosphorylation (Image 1) and is explained in reference 8.
Quoted From reference 8.
Trained innate immunity (TI) involving foamy macrophages and the production of high amounts of HERV-K102 particles is associated with the induction of glycolysis which is similar to the Warburg effect described for tumors. At the risk of being an oversimplification, a reason why glycolysis is needed for tumorigenesis (the Warburg effect) is so the mitochondria can produce the substrate acetyl-CoA/citrate (from glycolysis) needed for cholesterol production through the mevalonate pathway [17]. Replenishing of the cell surface membrane and other membranes in the cell via higher cholesterol production would be needed in order to support tumor proliferation. Indeed, mevalonate initiates DNA synthesis and cell proliferation [17]. In human monocyte derived macrophages, which incidentally do not proliferate, excess cholesterol would be needed and utilized instead for foam cell formation pertaining to the replication of the protector foamy virus HERV-K102. Hence, glycolysis is linked to TI to support the generation of foam (HERV-K102 particles and vacuoles) during macrophage immune training.
The lipid bodies (esterified cholesterol) that stain with Oil Red O in Image 2 may signify that there may be a higher risk of elevated oxidative stress in mitochondria causing dysfunction which contributes to corticosteroid resistance and thus an increased risk of PICS and CIRCI according to Drs. Meduri and Chrousos [3]. As well it is known that insulin resistance also pertains to mitochondrial dysfunction [18].
Thus, dysfunctional mitochondria and M2-like polarization may be the common factor unifying the risk of severe COVID-19 disease (spike pathology) as may be related to hypertension and diabetes.
In this regard, in a mouse model, dysfunctional mitochondria in the liver induces AFP (and the release of copper) that with copper activates cell death in CD8 T cells by (copper) activated AFP interacting with CCR5 [19].
(It is known that copper binds and activates AFP while zinc binds and inhibits AFP activity).
Recall that it is the heightened activity of alpha-fetoprotein (AFP) that drives immunosenescence in macrophages (ISM) and where only AFP antagonists can reverse or prevent ISM [4,5]. ISM causes chronic stress and/or age-associated diseases including cardiovascular disease, cancers, autoimmunity, metabolic syndrome, allergies, neurodegeneration, etc. This is related to the loss of DHEA with stress and/or aging that potentiates the action of cortisol by reducing the DHEA/cortisol ratio. Think of dehydroepiandrosterone (DHEA) as the youth hormone that counteracts the deleterious effects of cortisol in part by antagonizing the activity of AFP [4]. ISM is associated with a heightened risk of tumors/cancers and infectious diseases due to the loss of immunosurveillance associated with dysfunctional macrophages.
In terms of significance for SARS-CoV-2 spike related diseases, Patterson et al have demonstrated that CCR5 inhibition by maraviroc in critical COVID-19 patients decreases inflammatory cytokines, increases CD8 T-cells, and decreases SARS-CoV-2 RNA in plasma by day 14 promoting recovery [20].
Maraviroc is a drug which targets CCR5 and blocks CCR5 signaling, is known to reverse malignant potential and converts M2 macrophages to M1 (see Image 1) [21, 22].
However recovery from “post-acute sequelae of COVID-19” (PASC) in 18 PASC patients as also reported by Patterson et al [23] involved 6 to 12 weeks of 300 mg (twice daily) of maraviroc but with 10 mg daily of pravastatin and where the markers of vascular inflammation (sCD40L and VEGF) diminished associated with recovery.
These authors [23] suggest that the underlying illness causing PASC is vascular inflammation and not micro-clotting mediated in part via CCR5 and CX3CR1 (fractalkine receptor) on CD16+ (non-classical) monocytes. These monocytes bear spike S1 protein and are long lived because they are resistant to apoptosis [24]. They suggest that the statin inhibits endothelial inflammation and may be needed to block CD16+ binding to endothelial cells via CX3CR1 which also causes inflammation.
However the highest levels of CCR5 and CX3CR1 are on the intermediate monocytes (CD14+CD16+) which are the progenitors to the Lipid Body negative Foamy Macrophages (LB-FMs) referred to as the WDR74 positive macrophages [10] which SARS-CoV-2 converts to LB+FMs during severe COVID-19 (Image 2) in the lungs [8]. Moreover in earlier papers with 121 PASC patients, the only difference between PASC and healthy controls was elevated B cells and elevated CD14+CD16+ intermediate monocytes while both the intermediate and non-classical C16+ monocytes had cell surface S1 protein shown by flow cytometry [25].
Perhaps then, spike protein targets the C14+CD16+ intermediate monocytes and converts them to the CD16+ non-classical monocytes in analogy to what happens to the macrophages in the tissues (Images 1 and 2).
In terms of the contribution of statin to the recovery in PASC patients, statins do improve endothelial cell function, have antioxidant and anti-thrombotic actions and may increase mitochondrial apoptosis [26]. Thereby, statins by reducing the risks of mitochondrial oxidative stress may reduce glucocorticoid and insulin resistance which might correlate with reduced AFP activity [19] and thus recovery such as from PASC.
CONCLUSIONs
From Images 1 & 2 and the above discussion, principles for the treatment of spike protein diseases including COVID-19, PASC, post-COVID-19 vaccination syndrome and even ‘turbo cancer’ emerges:
Decrease endothelial cell inflammation.
Decrease mitochondrial dysfunction and/or quench oxidative stress.
Antagonize the pathogenic effects of active AFP.
Eliminate sources of spike protein.
In addition to the Patterson Protocol of using a statin with maraviroc for 6 to 12 weeks [23] which is currently undergoing randomized clinical trial evaluation there are other steps to reduce the risks of developing PASC.
Accordingly, the following steps (no particular order) or considerations would be expected to help prevent onset of PASC and/or help promote recovery:
pre and pro biotics to flush out the allegedly contaminated bacteria in the gut that potentially might harboring the gene therapy mRNA and cDNA of the COVID-19 vaccines (directly injected COVID-19 vaccinees or via shedding to the unvaccinated) and ALSO to rebalance the microflora of the gut
nattokinase/bromelain to digest any S1 protein especially as the reservoir might be in the gut
ban the COVID-19 vaccines
ban the mRNA gene therapy “vaccine” technology which may cause the shedding of spike protein mRNA/cDNA in exosomes with dire consequences for the new host (see recent substack articles on shedding)
do not allow recently COVID-19 vaccinated to donate blood (and screen donors for spike protein) (never allow recent recipients of gene therapy to donate!)
top up Vit D3, C, B1 and consider NAC and near infrared exposures to help diminish the oxidative stress to help promote the recovery of glucocorticoid receptor alpha to reestablish homeostasis by diminishing glucocorticoid and insulin resistance
AFP antagonists to reverse ISM [4,5, 8] including: 7-keto-DHEA, Vitamin D3, zinc, isoflavones (genistein for example because the estrogen receptor regulates key hub genes in cancers, ISM and GC resistance [27]) and especially ivermectin [6] or as a potential substitute, artemisinin (early data are very encouraging but needs to be validated)
intermittent fasting to encourage toxin clearance
supplement daily with whey proteins (not plant proteins [28]) and a multivitamin [29]
avoid sugar and alcohol, adopt a healthy diet and be mindful of meeting BMIs of about 19 to 24 [29]
daily outdoor activities such as a 30 minute walk around noon to encourage vitamin D3 production [29], and
outdoor activities to enhance near infrared radiation exposures (goes through clothes) which actually generates intracellular melatonin in the mitochondria to counteract the oxidative stress of oxidative phosphorylation [30] which counterbalances spike protein’s ability to lead to CIRCI and continued disease.
In certain cases a second or third line of therapy using low dose glucocorticoid therapy (methylprednisolone [31]) might be needed for recovery as suggested in the I-Recovery Protocols for long COVID and post-vaccination treatment guides of the FLCCC [32].
References
Chacin-Bonilla, L. and Bonilla, E. 2023. Melatonin and Covid-19: An opened Pandora’s box and the hope for the time being. Melatonin Research. 6, 4 (Dec. 2023), 474-484. DOI:https://doi.org/https://doi.org/10.32794/mr112500163.
Zhou Y, Zhang T, Wang X, Wei X, Chen Y, Guo L, Zhang J, Wang C. Curcumin Modulates Macrophage Polarization Through the Inhibition of the Toll-Like Receptor 4 Expression and its Signaling Pathways. Cell Physiol Biochem. 2015;36(2):631-41. doi: 10.1159/000430126.
Meduri GU, Chrousos GP. General Adaptation in Critical Illness: Glucocorticoid Receptor-alpha Master Regulator of Homeostatic Corrections. Front Endocrinol (Lausanne). 2020 Apr 22;11:161. doi: 10.3389/fendo.2020.00161.
Laderoute MP. A new paradigm about HERV-K102 particle production and blocked release to explain cortisol mediated immunosenescence and age-associated risk of chronic disease. Discov Med. 2015 Dec;20(112):379-91.
Laderoute M. The paradigm of immunosenescence in atherosclerosis-cardiovascular disease (ASCVD). Discov Med. 2020 Jan-Feb;29(156):41-51.
Laderoute M. Ivermectin may prevent and reverse immunosenescence by antagonizing alpha-fetoprotein and downmodulating PI3K/Akt/mTOR hyperactivity. Open Heart, April 29, 2021. https://openheart.bmj.com/content/8/1/e001655.responses#ivermectin-may-prevent-and-reverse-immunosenescence-by-antagonizing-alpha-fetoprotein-and-downmodulating-pi3k-akt-mtor-hyperactivity.
Peluso MJ et al., medRxiv preprint v.3 December 29, 2023.
Laderoute, M. Antibody Dependent Enhancement (ADE) of Infection into Macrophages Validates the Importance of HERV-K102 Particle Production for Pandemic Preparedness. Preprints 2023, 2023120185. https://doi.org/10.20944/preprints202312.0185.v1
See version 2 below.
Ziegler CGK, Miao VN, Owings AH, et al. Impaired local intrinsic immunity to SARS-CoV-2 infection in severe COVID-19. Cell. 2021 Sep 2;184(18):4713-4733.e22. doi: 10.1016/j.cell.2021.07.023.
Ren X, Wen W, Fan X, et al. COVID-19 immune features revealed by a large-scale single-cell transcriptome atlas. Cell. 2021 Apr 1;184(7):1895-1913.e19. doi: 10.1016/j.cell.2021.01.053.
Fisman DN, Tuite AR. Evaluation of the relative virulence of novel SARS-CoV-2 variants: a retrospective cohort study in Ontario, Canada. CMAJ. 2021 Oct 25;193(42):E1619-E1625. doi: 10.1503/cmaj.211248.
Geng J, Chen L, Yuan Y, Wang K, Wang Y, Qin C, Wu G, Chen R, Zhang Z, Wei D, Du P, Zhang J, Lin P, Zhang K, Deng Y, Xu K, Liu J, Sun X, Guo T, Yang X, Wu J, Jiang J, Li L, Zhang K, Wang Z, Zhang J, Yan Q, Zhu H, Zheng Z, Miao J, Fu X, Yang F, Chen X, Tang H, Zhang Y, Shi Y, Zhu Y, Pei Z, Huo F, Liang X, Wang Y, Wang Q, Xie W, Li Y, Shi M, Bian H, Zhu P, Chen ZN. CD147 antibody specifically and effectively inhibits infection and cytokine storm of SARS-CoV-2 and its variants delta, alpha, beta, and gamma. Signal Transduct Target Ther. 2021 Sep 25;6(1):347. doi: 10.1038/s41392-021-00760-8.
Shrestha NK, Burke PC, Nowacki AS, Simon JF, Hagen A, Gordon SM. Effectiveness of the coronavirus disease 2019 bivalent vaccine. Open Forum Infect Dis. 2023 Apr 19;10(6):ofad209. doi: 10.1093/ofid/ofad209.
Oh J, Weng S, Felton SK, et al. 1,25(OH)2 vitamin D inhibits foam cell formation and suppresses macrophage cholesterol uptake in patients with type 2 diabetes mellitus. Circulation. 2009 Aug 25;120(8):687-98. doi: 10.1161/CIRCULATIONAHA.109.856070.
Dias SSG, Soares VC, Ferreira AC, et al. Lipid droplets fuel SARS-CoV-2 replication and production of inflammatory mediators. PLoS Pathog. 2020 Dec 16;16(12):e1009127. doi: 10.1371/journal.ppat.1009127.
Coleman PS, Parlo RA. Warburg's ghost-cancer's self-sustaining phenotype: the aberrant carbon flux in cholesterol-enriched tumor mitochondria via deregulated cholesterogenesis. Front Cell Dev Biol. 2021 Mar 12;9:626316. doi: 10.3389/fcell.2021.626316.
Sangwung P, Petersen KF, Shulman GI, Knowles JW. Mitochondrial Dysfunction, Insulin Resistance, and Potential Genetic Implications. Endocrinology. 2020 Apr 1;161(4):bqaa017. doi: 10.1210/endocr/bqaa017.
Jett KA, Baker ZN, Hossain A, Boulet A, Cobine PA, Ghosh S, Ng P, Yilmaz O, Barreto K, DeCoteau J, Mochoruk K, Ioannou GN, Savard C, Yuan S, Abdalla OH, Lowden C, Kim BE, Cheng HM, Battersby BJ, Gohil VM, Leary SC. Mitochondrial dysfunction reactivates α-fetoprotein expression that drives copper-dependent immunosuppression in mitochondrial disease models. J Clin Invest. 2023 Jan 3;133(1):e154684. doi: 10.1172/JCI154684.
Patterson BK, Seethamraju H, Dhody K, Corley MJ, Kazempour K, Lalezari J, Pang APS, Sugai C, Mahyari E, Francisco EB, Pise A, Rodrigues H, Wu HL, Webb GM, Park BS, Kelly S, Pourhassan N, Lelic A, Kdouh L, Herrera M, Hall E, Bimber BN, Plassmeyer M, Gupta R, Alpan O, O'Halloran JA, Mudd PA, Akalin E, Ndhlovu LC, Sacha JB. CCR5 inhibition in critical COVID-19 patients decreases inflammatory cytokines, increases CD8 T-cells, and decreases SARS-CoV2 RNA in plasma by day 14. Int J Infect Dis. 2021 Feb;103:25-32. doi: 10.1016/j.ijid.2020.10.101.
Zhuang Y, Zhao X, Yuan B, Zeng Z, Chen Y. Blocking the CCL5-CCR5 Axis Using Maraviroc Promotes M1 Polarization of Macrophages Cocultured with Irradiated Hepatoma Cells. J Hepatocell Carcinoma. 2021 Jun 18;8:599-611. doi: 10.2147/JHC.S300165.
Xu J, Shi Q, Lou J, Wang B, Wang W, Niu J, Guo L, Chen C, Yu Y, Huang Y, Guo W, Lan J, Zhu Y, Ren T, Tang X. Chordoma recruits and polarizes tumor-associated macrophages via secreting CCL5 to promote malignant progression. J Immunother Cancer. 2023 Apr;11(4):e006808. doi: 10.1136/jitc-2023-006808.
Patterson BK, Yogendra R, Guevara-Coto J, Mora-Rodriguez RA, Osgood E, Bream J, Parikh P, Kreimer M, Jeffers D, Rutland C, Kaplan G, Zgoda M. Case series: Maraviroc and pravastatin as a therapeutic option to treat long COVID/Post-acute sequelae of COVID (PASC). Front Med (Lausanne). 2023 Feb 8;10:1122529. doi: 10.3389/fmed.2023.1122529.
Patterson BK, Francisco EB, Yogendra R, Long E, Pise A, Rodrigues H, Hall E, Herrera M, Parikh P, Guevara-Coto J, Triche TJ, Scott P, Hekmati S, Maglinte D, Chang X, Mora-Rodríguez RA, Mora J. Persistence of SARS CoV-2 S1 Protein in CD16+ Monocytes in Post-Acute Sequelae of COVID-19 (PASC) up to 15 Months Post-Infection. Front Immunol. 2022 Jan 10;12:746021. doi: 10.3389/fimmu.2021.746021.
Patterson BK, Guevara-Coto J, Yogendra R, Francisco EB, Long E, Pise A, Rodrigues H, Parikh P, Mora J, Mora-Rodríguez RA. Immune-Based Prediction of COVID-19 Severity and Chronicity Decoded Using Machine Learning. Front Immunol. 2021 Jun 28;12:700782. doi: 10.3389/fimmu.2021.700782.
Mollazadeh H, Tavana E, Fanni G, Bo S, Banach M, Pirro M, von Haehling S, Jamialahmadi T, Sahebkar A. Effects of statins on mitochondrial pathways. J Cachexia Sarcopenia Muscle. 2021 Apr;12(2):237-251. doi: 10.1002/jcsm.12654.
Chen Y, Jiang P, Wen J, Wu Z, Li J, Chen Y, Wang L, Gan D, Chen Y, Yang T, Lin M, Hu J. Integrated bioinformatics analysis of the crucial candidate genes and pathways associated with glucocorticoid resistance in acute lymphoblastic leukemia. Cancer Med. 2020 Apr;9(8):2918-2929. doi: 10.1002/cam4.2934.
Rajamohan T, Kurup PA. Lysine: arginine ratio of a protein influences cholesterol metabolism. Part 1--Studies on sesame protein having low lysine: arginine ratio. Indian J Exp Biol. 1997 Nov;35(11):1218-23.
Laderoute MP. “The HERV-K Way to Keep Coronavirus at Bay”. Originally posted to LinkedIn March 5, 2020 but after being banned, reposted to my substack: on February 26, 2022.
The HERV-K Way to Keep Coronavirus (COVID-19) at Bay
·
IMAGE: The meaning of the HERV-K acronym. Given that the stealth omicron variant is gaining foothold internationally and may be 30% more transmissible that the original omicron variant, it is important to remember that pre-existing immunosenescence remains the key risk factor for COVID-19 severity. In addition accumulating evidence strongly suggests th…
Zimmerman, S. and Reiter, R. 2019. Melatonin and the Optics of the Human Body. Melatonin Research. 2, 1 (Feb. 2019), 138-160. DOI:https://doi.org/https://doi.org/10.32794/mr11250016.
Salton F, Confalonieri P, Meduri GU, Santus P, Harari S, Scala R, Lanini S, Vertui V, Oggionni T, Caminati A, Patruno V, Tamburrini M, Scartabellati A, Parati M, Villani M, Radovanovic D, Tomassetti S, Ravaglia C, Poletti V, Vianello A, Gaccione AT, Guidelli L, Raccanelli R, Lucernoni P, Lacedonia D, Foschino Barbaro MP, Centanni S, Mondoni M, Davì M, Fantin A, Cao X, Torelli L, Zucchetto A, Montico M, Casarin A, Romagnoli M, Gasparini S, Bonifazi M, D'Agaro P, Marcello A, Licastro D, Ruaro B, Volpe MC, Umberger R, Confalonieri M. Prolonged Low-Dose Methylprednisolone in Patients With Severe COVID-19 Pneumonia. Open Forum Infect Dis. 2020 Sep 12;7(10):ofaa421. doi: 10.1093/ofid/ofaa421.
https://covid19criticalcare.com/protocol/i-recover-long-covid-treatment/
https://covid19criticalcare.com/protocol/i-recover-post-vaccine-treatment/


Thank You again, Dr. Laderoute. The revision is much clearer.
Here is another paper showing that active AFP causes the shift from M1 to Mw : Zhang M, Liu K, Zhang Q, Xu J, Liu J, Lin H, Lin B, Zhu M, Li M. Alpha fetoprotein promotes polarization of macrophages towards M2-like phenotype and inhibits macrophages to phagocytize hepatoma cells. Front Immunol. 2023 Feb 23;14:1081572. doi: 10.3389/fimmu.2023.1081572.