


Is being vaccinated by spike mRNA gene therapy shots at large indoor clinics treacherous?
Was there any Informed Consent on this Issue?

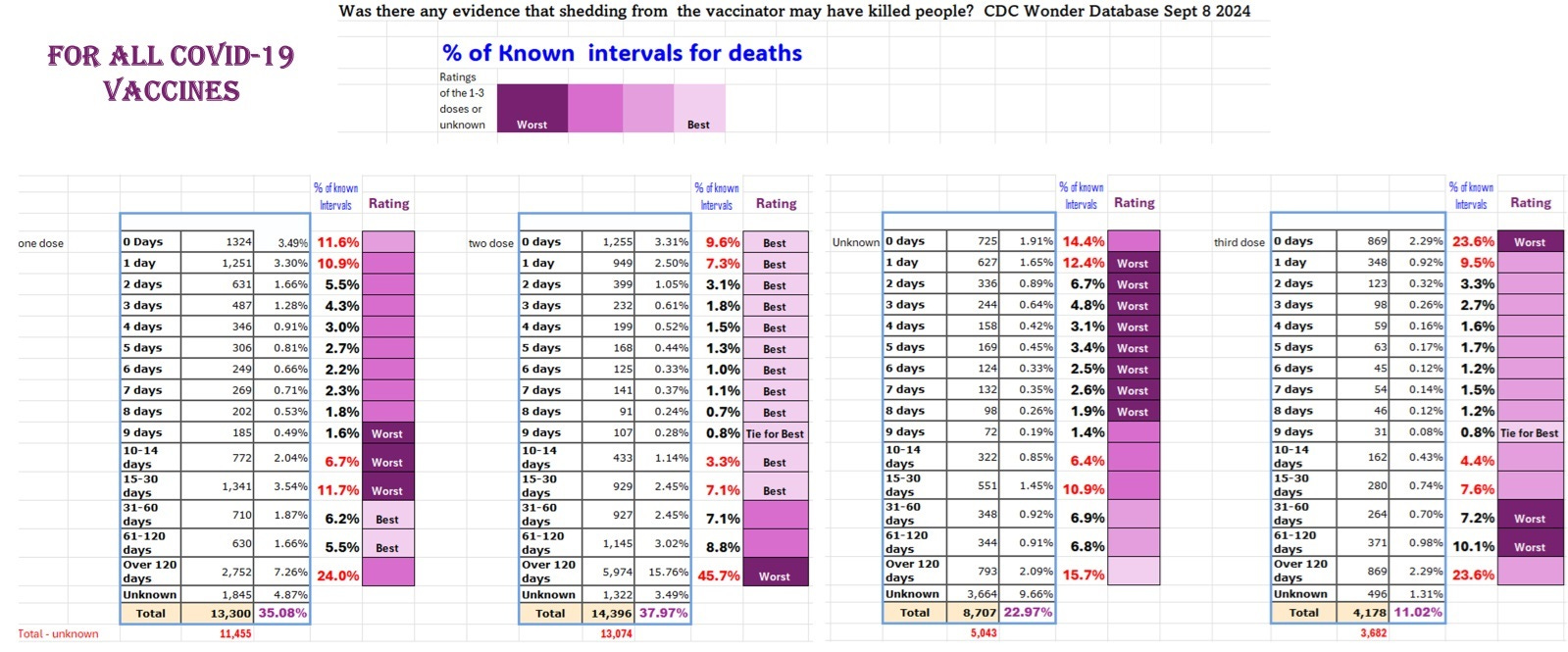
Image 1. VAERS DEATH data (CDC Wonder database) for COVID-19 Spike Vaccines by Onset Interval by Dose
Generally speaking we see a pattern of significant mortality at up to 24 hours (early mortality) and then again at around 120 days (late mortality).
The issue is raised here that the early mortality could be due to hitting a vein (accidental inoculation i.v.), allergies to components of vaccines for example involving anti-PEG and mRNA shots, direct toxicity of mRNA or cDNA shots, and/or shedding from the vaccinator if they received 2 doses of the spike mRNA vaccines in the past 3 months.
For the late mortality, it could be largely due to shedding from recently spike mRNA vaccinated after the second dose (ie., estimated to persist for up to three months). Note that the relative highest late mortality was indeed after the second shot as was reported to VAERS.
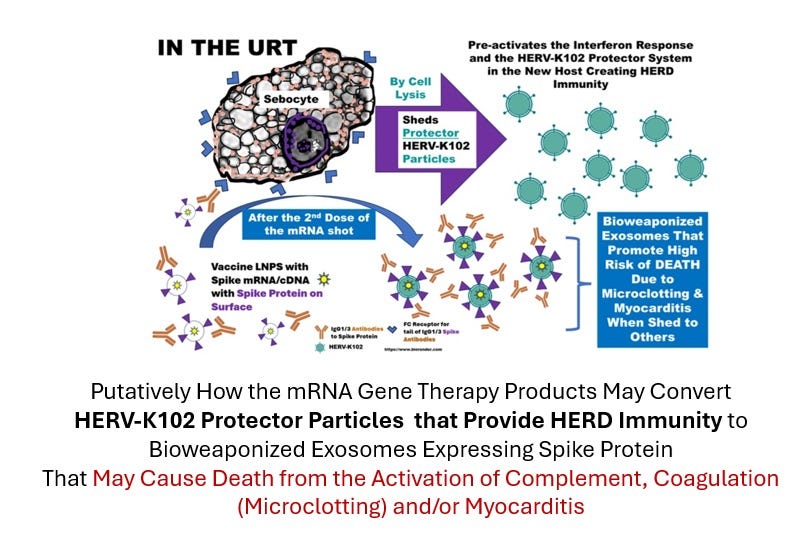
Image 2. How the Spike mRNA Shots Create Bioweaponized CD9 Positive Exosomes That are Exhaled
It was recently proposed [1] that after the second dose with process two lipid nanoparticles (LNPs) which putatively are laden with spike protein on the surface (unlike process one where it is impossible for the production of spike protein) these become targeted to the foamy macrophages through spike IgG1/3 via the FCGR2A. This targeting in the upper respiratory tract means the sebocytes of sebaceous glands in the mucosa (which are highly specialized foamy macrophages) are highly transfected, and produce the spike laden CD9 exosomes [2] which we know are derived from macrophages [3]. Judging by the protein contents of the CD9 exosomes during mild versus severe COVID-19 [3], the CD9 exosomes are most likely the protector HERV-K102 particles {same size for example and same source ie., activated M1 like, lipid body negative foamy macrophages producing IL1B, IL-6, TNF and the HERV-K102 particles, see Image 3).
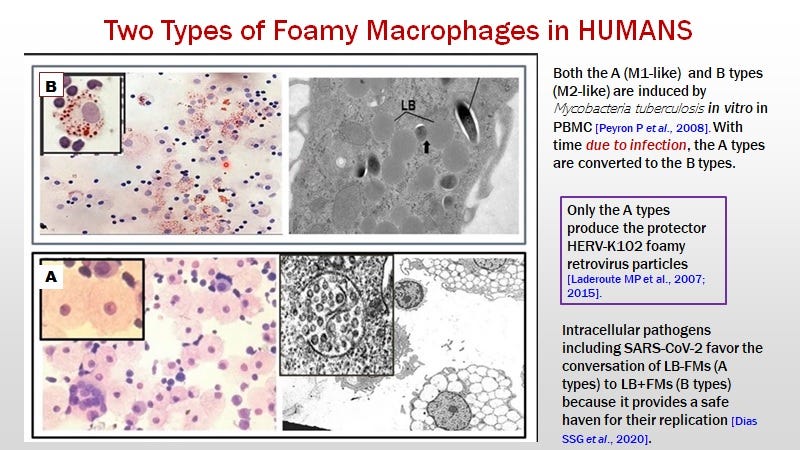
Image 3. Two Types of Foamy Macrophages: Only the O Red Oil Negative Produce the Protector HERV-K102 Particles Associated with M1 -Like Programming
For dose 1 it was known that attendance at the large indoor immunization venues was associated with catching SARS-CoV-2. This explains the relative increase in death at 9 to 30 days (ie., the worst category) when compared to the other doses and the unknown dose categories. Subsequently at 30 to 120 days, the trained innate immunity induced by dose 1, reduced all-cause mortality so here, the relative risk of death is lowest (compared to the other doses or unknown category).
For the second dose, the relative risk of death is quite favorable for the first 30 days when compared with other doses due to the massive secondary response of trained innate immunity which is thought to strongly induce innate T and B cells responses to HERV-K102 envelope in addition to high levels of HERV-K102 particles (10 to the power of 12)[4]. Because the SARS-CoV-2 virus is enveloped it means as it buds from the cell surface it picks up the HERV-K102 envelope (conformationally distinct from the particle envelope and there are some amino acid differences) which is a surrogate marker of virus infected cells. Therefore these innate antibodies are capable of neutralizing and clearing SARS-CoV-2 virions and the relative risk of death goes down [4]. From day 31 to 120, there is a moderate relative increase in risk of death, as the lipid body negative foamy macrophages are converted to the lipid body positive dysfunctional foamy macrophages (see Image 4).
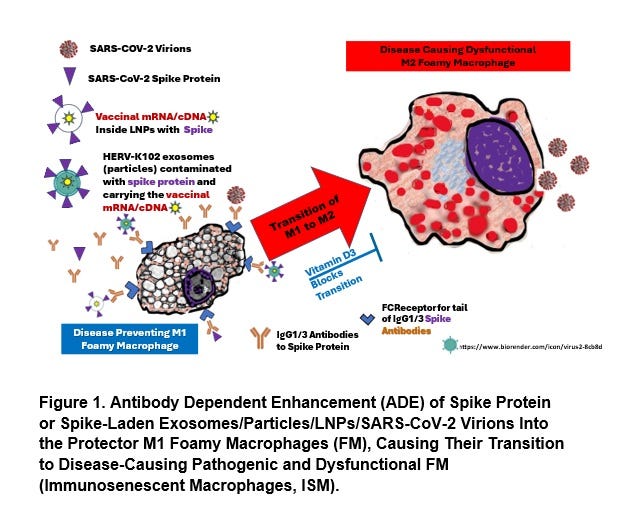
Image 4. Via ADE Involving Spike IgG1/3, the Spike mRNA Shots Wipe Out Innate Immunity (Except NOT in Individuals with Optimal Vitamin D3)
However, due to the common shedding of the bioweapons for up to 3 months after the second dose mRNA vaccination (Image 2), the highest risk for mortality is indeed after 120 days after the second shot. These individuals will retain the spike IgG1/3 for at least 3 months placing them at high risk. People who were infected with SARS-CoV-2 prior to receiving the mRNA shots will not convert to IgG4 by 6 months or with the 3rd dose and thus, REMAIN AT THE HIGHEST RISK OF SHEDDING WHICH INVOLVES SUDDEN DEATH. Accordingly, medical personnel are in this category because most would have been exposed prior to the mRNA shot availability. Younger people received the mRNA shots after the elderly so also they were more likely to have been infected before receiving the mRNA shots when compared with the elders. These findings help explain how the healthy young athletes succumbed to sudden deaths as well as nurses and MDs.
At the time of the third dose, the early mortality rate is highest. In fact the heightened risk of death is within the first 24 hours strongly suggesting the vaccinators may be highly shedding. It is important to remember that the IgG1/3 antibodies in the upper respiratory tract, do NOT apparently convert to IgG4 no matter how many shots are given [4]. So when they got their 3rd dose (right before administering the 3rd dose to others) they are spewing the potent bioweapons where ever they go. This may be the strongest evidence for the potential risk of vaccinators on the vaccinated when spike mRNA shots are given.
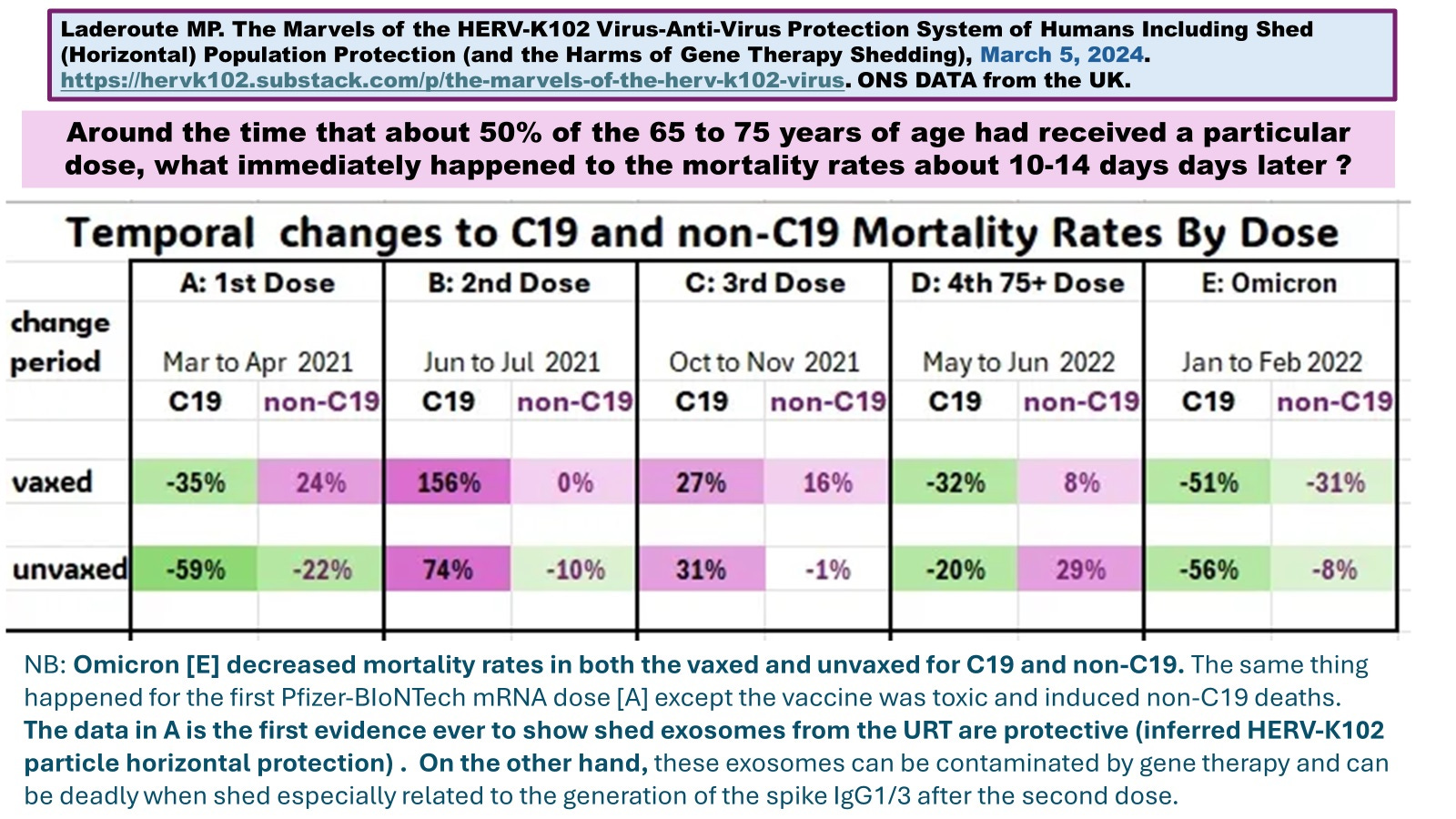
Image 5. The Shed Protection of HERV-K102 Particles Against Non-COVID-19 Mortality Progressively Diminishes with Each Dose in the Unvaccinated Suggesting with Each Dose There are MORE Potent Bioweapons Being Produced
For the third dose, at 31 to 120 days there appears to be an increased risk of deaths relative to the other doses, possibly due to being shed upon by others.
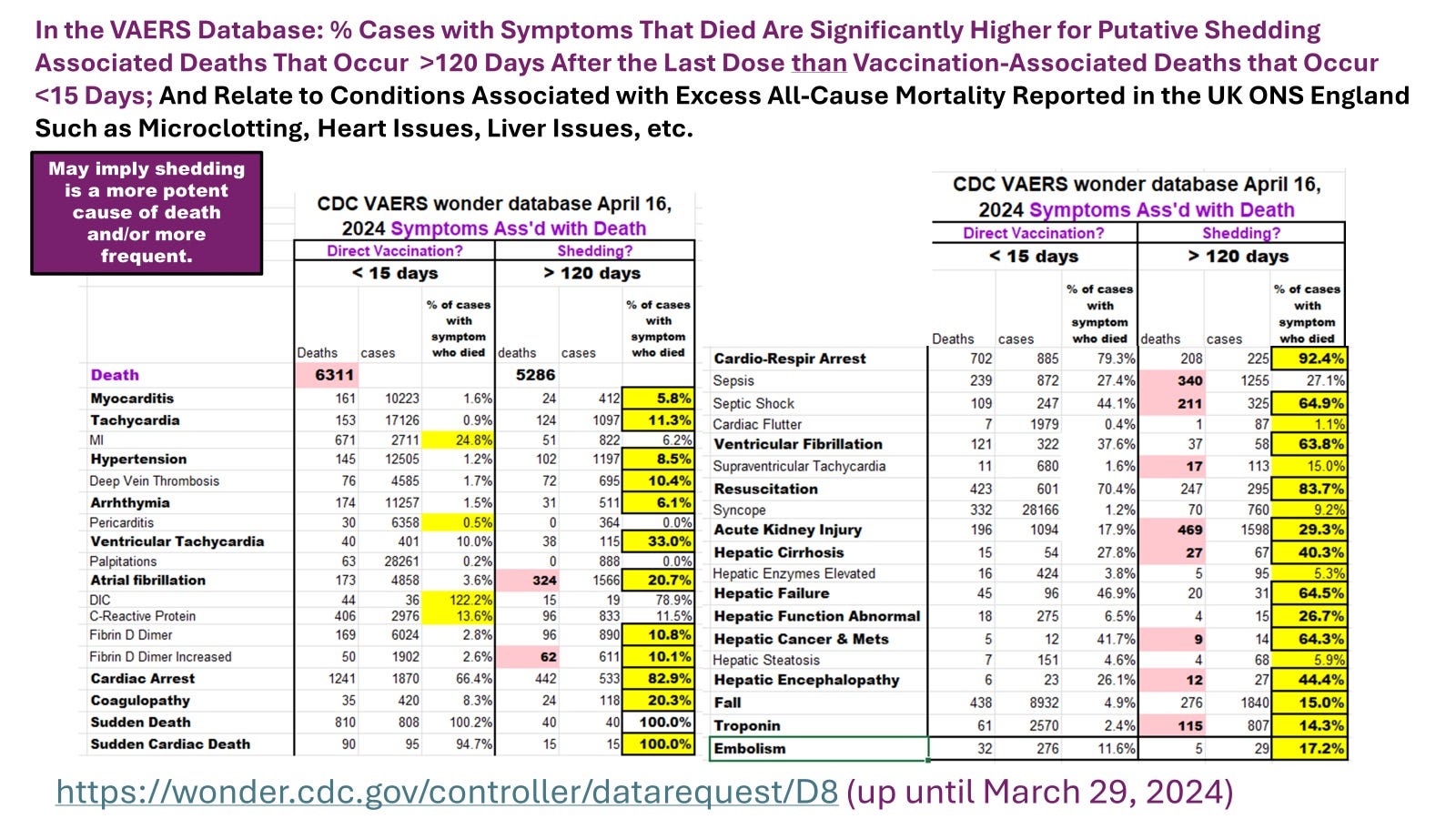
Image 6. In Individuals with Symptoms Related to Microclotting, There is a Greater Risk of Death at >120 Days (Case Fatality Rates Are Higher) than Within the First 15 Days, But the Incidence of These Symptoms is Much Higher in the Early Cases
NB: Some of the late cases reported to VAERS involved reinfection with SARS-CoV-2 which contributes strongly to the death. Nevertheless population data from England where SARS-CoV-2 infection would count as a COVID-19 death, the risk of shedding causing a non-COVID death was about 9-fold higher (>63 days) than the direct vaccination risk of death (<15 days) [1].
CONCLUSIONS
Most people were aware of people catching SARS-CoV-2 at the large indoor clinics when they presented for the first dose. The data reviewed here may be first to suggest the potential existence of the shedding risk of the recently vaxed vaccinator causing death.
REFERENCES:
https://rumble.com/v51idm2-dr.-marian-laderoute-jun-01-2024-regina-saskatchewan.html
Bansal S et al., J Immunology, November 15, 2021.
Pesce E et al., Frontiers in Immunology, Jan 17, 2022.
Laderoute, M. Antibody Dependent Enhancement (ADE) of Infection into Macrophages Validates the Importance of HERV-K102 Particle Production for Pandemic Preparedness. Preprints 2023, 2023120185. https://www.preprints.org/manuscript/202312.0185/v2.
DOI: 10.20944/preprints202312.0185.v2.
Thank you for this data! It confirms what I experienced. All of my clients, except one, are vaxxed. As an unvaxxed, sensitive person, I have been so sick with “upper respiratory illnesses” and/or other “viral” symptoms ever since the bioweapons were deployed, including this summer after a couple clients faithfully for boosted for the 6th, 7th or 8th time!As a cleaner, I’m constantly breathing in their shedding.
I need to start asking if they’ve been boosted and demand seeing their cards so I can drop them as clients.
Peter McCullough MD, Anti-Spike Antibodies Among Vaccinated Predict Major Adverse Events after Myocardial Infarction
Lab Test Indirectly Implicates Spike as Cause of Complications after Heart Attack
https://petermcculloughmd.substack.com/p/anti-spike-antibodies-among-vaccinated