

A Call to Arms
A Call to Arms
Revision Sept 24, 2023 showing 3rd dose mitigates the risk of ADE but is NOT as safe as being unvaccinated (based on all-cause mortality rate ratios).

Yesterday, Dr. John Campbell’s webinar was about Sudden Adult Deaths (SAD) that contribute to excess all-cause mortality (EACM) in highly vaccinated countries. He was careful to point out that this seemed to be those countries in which the majority of citizens had been vaccinated with one or two doses.

Recently Dr. Steve Pelech, the Co-Chair of the Scientific and Medical Advisory Committee of the Canadian Covid Care Alliance sent me his graphs of the UK ONS mortality data (18+) by vaccination status covering April 2021 - December 2022 (Figure 1) for deaths after 21 days after the last dose.

Figure 1. UK ONS Data Reveals The Third Dose Was Consistently Associated with the LEAST COVID-19 and non-COVID-19 Mortality:
However this is only when the data are compared which “excluded deaths during first 21 days” after vaccination. This is a major caveat of Figure 1.
When the data are inclusive of what happens in the first 21 days after vaccination, the all-cause mortality risk of the 3rd dose is generally higher than the unvaccinated as shown here for the 50 + by age group for February 2022 in the Table (below). Even though the 3rd dose for the 50-59 has a comparable risk to no doses of vaccines, the higher risk of two doses precludes the benefit of the third dose.
In other words despite the 3rd dose neutralizing the adverse effects of ADE on mortality outcomes, the mRNA gene therapy injections are so toxic, that this risk negatively generates very high all-cause mortality. These mRNA gene therapy injections MUST stop!

Data from: Office for National Statistics (ONS UK). Deaths involving COVID-19 by vaccination status, England: Deaths occurring between 1 January 2021 and 31 May 2022. Age-standardised mortality rates and raw death numbers for deaths involving COVID-19 by vaccination status, broken down by age and /or sex group. RELEASED July 6, 2022. https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/deaths/bulletins/deathsinvolvingcovid19byvaccinationstatusengland/deathsoccurringbetween1january2021and31may2022.
NB: The third mRNA Covid vaccine dose in which the harmful spike specific IgG1/3 that mediates antibody dependent enhancement (ADE) of infection into macrophages is converted to non-harmful IgG4 [Irrgang P et al., 2022; Uversky VN et al., 2023; Kiszel P et al., 2023], provides neutralization against all-cause mortality in those who received one or two doses of vaccine (Figure 1 and Table).
This provides direct proof consistent with the notion that the risk of COVID-19 and non-COVID-19 mortality relates to antibody dependent enhancement (ADE) of SARS-CoV-2 infection into the foamy macrophages (COVID-19 mortality) or spike protein triggering/entry into foamy macrophage (non-COVID-19 mortality) promoting immunosenescence of macrophages.
These data galvanizes the notions that
1) the activation of “trained INNATE immunity” in foamy macrophages is critical to the clearance of SARS-CoV-2 and,
2) foamy macrophages made dysfunctional by exposures to spike protein probably involves immunosenescence which increases the risk not only of infectious diseases and cancers but also cardiovascular, neurological and autoimmune diseases [Laderoute MP, 2015; 2020].
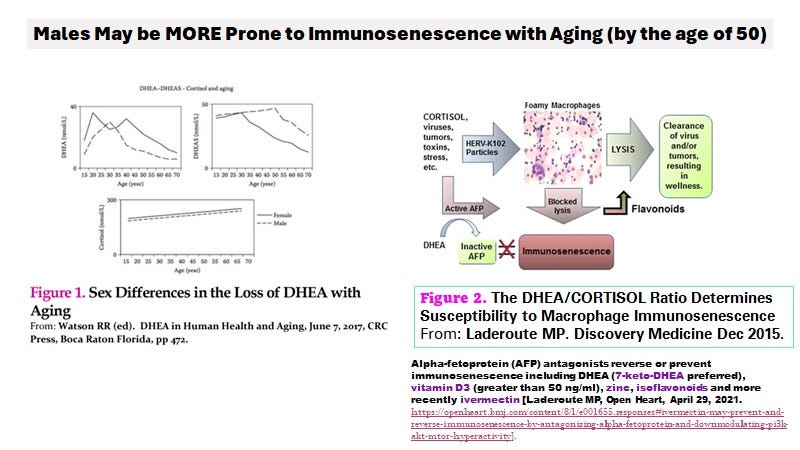
Figure 2. Low DHEA Levels in Males might Correlate with i) immunosenescence risk and/or ii) EACM risks
Note that DHEA (active) but not DHEAS (inactive) binds and inactivates (AFP) [Laderoute MP. Discovery Medicine, Dec 2015]. When DHEA levels are too low for the amount of cortisol, this means more of the AFP will be active upon the activation of monocytes-macrophages by viruses, by lipid nanoparticles, by foreign DNA/RNA, and/or toxic spike protein. Active but not inactive AFP causes immunosenescence of macrophages, so the loss of DHEA with earlier age in males places them at much higher risk of immunosenescence.
NB: the omicron and subvariants are very transmissible in C19 vaccinated population (see Cleveland data) and infection rates increase proportionately to C19 vaccine doses. Maybe the transformation of spike IgG1/3 to IgG4 does not occur in the URT (?). At any rate, it is possible there might be many subclinical infections with omicron subvariants which is why these deaths are labelled as non-COVID-19 deaths. I suspect many of the EACM relates to some SARS-CoV-2 circulating. For others it is the persistence of spike protein and/or the foreign RNA/DNA persisting in the host. It could be if macrophages finally lyse, they may spill the foreign material which increases the likelihood of an adverse event. Clearly we need to determine if there are risk factors which would indicate who should be on a prevention protocol.
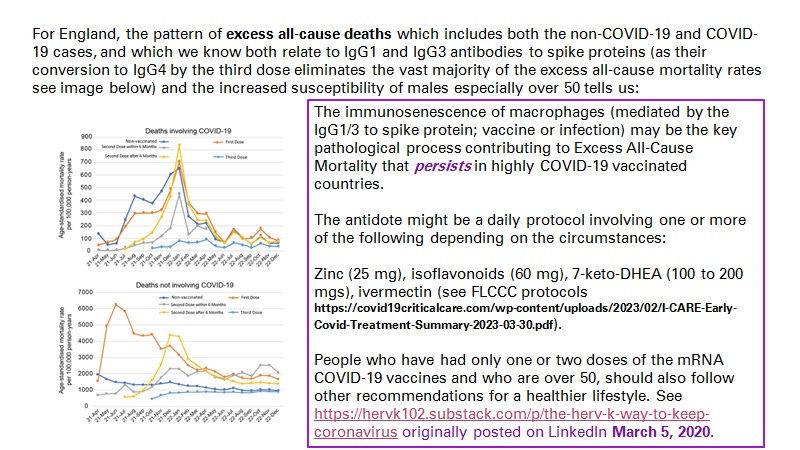
Figure 3. Potential Antidotes to EACM Risks in Those over 50 Years of Age and who have only received one or two doses of COVID-19 mRNA vaccines
The potential upcoming loss of potentially more than 63,000 UK citizens due to 1) experimental use of toxic and lethal mRNA gene therapy injections authorized for administration to healthy children and adults including pregnant moms all without any significant safety studies; and 2) COVID-19 vaccines administered without consideration of the extreme dangers of ADE related to adaptive immunity antibodies, has been an undeniably diabolical assault on mankind.
Since formal government sponsored public health authorities are not providing risk assessment, let alone risk management strategies despite hefty tax payer dollar support, it is incumbent on decent knowledgeable people to meet and discuss how best to remedy this situation. Given the illuminating data originates in the UK, perhaps Dr. Tess Lawrie from the World Council for Health (an expert in risk estimation) would lead the discussion. There are many issues to discuss and very little time, before the respiratory virus season descends upon us in the northern hemisphere.
Items to be discussed would include:
likelihood that ensuring vitamin D blood levels at above 50 ng/ml would suffice to quench both COVID and non-COVID-19 excess mortality; if so, issuing an advisory guidance by the World Council for Health;
what additional protocols might be useful and why, including an assessment of ivermectin in preventing death;
do hybrid vaccines continue to create excess mortality?
what are the most common “causes” or symptoms of increased risk and is there a separate screening test (eg., hypertension, D-dimers, CRP, or atrial fibrillation) to identify those who may be at increased risk and who may benefit from ivermectin and/or nattokinase;
how much of the risk relates to immunosenescence of macrophages?
the need and planning for testing for IgG isotypes of spike specific antibodies by vaccination status (comparing Wuhan vs hybrid booster vaccines ) and infection status (pre and post vaccination) in blood versus saliva;
would offering a 3rd dose be needed? {if the benefits versus risks are acceptable for some people} ; and
so on.

Figure 4. Moderna Myocarditis Signal is Also Reduced with the Third Dose Implying ADE Plays a Major Role in Myocarditis (from Patone M et al, August 22, 2022).
Note the last column refers to those who were vaccinated then infected with SARS-CoV-2 (?).
Additionally I have attached graphs from the Office for Health Improvement and Disparities (OHID) on the causes associated with the excess mortality (predominantly circulatory causes (some but not a lot of cancer?) consistent with immunosenescence of macrophages which may cause hypertension and cardiovascular diseases) as copied from:
Hypertension is a sign/symptom of immunosenescence of macrophages related to ACE activity in the activated foamy macrophages (FM). However, since the FMs cannot lyse to release the protector HERV-K102 particles, they persist in the host and there is a build up of blood pressure. The immunosenescence paradigm was specifically validated for cardiovascular disease in 2020 [Laderoute M. The paradigm of immunosenescence in atherosclerosis-cardiovascular disease (ASCVD). Discov Med. 2020 Jan-Feb;29(156):41-51. ]. Most causes linked to the excess all-cause mortality following mass C19 vaccination involve the circulation according to the OHID for England, and would be consistent with excess mortality reflective of the immunosenescence of macrophages.
Very interesting perspective on the role of IgG4 in all of this. I'll try to see if there are others arriving to the same conclusion within the literature.
Thank you for sharing, take care!