

Why was the mortality rate for the SARS-CoV-2 omicron variant wave higher than delta for many high vaccinating countries and lower for slow vaccinating countries?
Why was the mortality rate for the SARS-CoV-2 omicron variant wave higher than delta for many high vaccinating countries and lower for slow vaccinating countries?
The case for vaccine promoted COVID-19 deaths during the omicron wave.

March 9 2022. V5.
It serves me no pleasure in reporting this analysis.
Not only did global public health authorities not heed the similar mistakes documented for small pox pandemics in the 1800’s, but they ignored the early warnings by Dr. Geert Vanden Bossche a well seasoned vaccinologist, that you cannot use adaptive immunity vaccination to stop an emerging pandemic RNA virus. Another Belgian scientist, Dr. Marc Wathelet, an expert in coronavirus effects on immunity, pleaded with the Belgium government to offer ivermectin for 2 weeks for its citizens and thereafter the test and treat strategy to reduce the upcoming expected morbidity and mortality with the novel emerging coronavirus. Both were ignored.
Why are adaptive immunity vaccines potentially harmful against emerging RNA virus pandemics? Why are neutralizing antibodies to spike protein dangerous?
Since it takes at least full two weeks or more for humans to make sufficient neutralizing antibody against an RNA virus that it has never seen before, highly pathogenic emerging viruses can kill the host before this. If the virus is less virulent, as antibody levels rise to sufficient levels, there would have already been selection for escape mutants. This is because RNA viruses notoriously exist in swarms or pools of variants due to poor proofreading while their RNA genomes are being replicated. Thus the adaptive immune system gets caught in a dangerous game of producing antibody to the strain of 10 days ago, never catching up. Thus the adaptive immune system makes a futile attempt to protect the human host all the time selecting for immune escape mutants and increasing the risk of antibody dependent enhancement (ADE) of infection and pathogenesis. This ADE is believed to largely involve the FCGR2A upregulated on macrophages and neutrophils, but may also involve FCGR3A as may be upregulated on dendritic cells and perhaps subtypes of B cells. The entry of the virus into these key protector cells serves to abrogate or silence the host protection mechanisms and render the cells dysfunctional.
In COVID-19, Virus Specific Antibodies Correlate with Severity Rather Than Protection
According to Lee et al [Lee WS et al., Nature Microbiology October 2020] for COVID-19: “you know you are going to have a problem with ADE related to adaptive immunity vaccines if the IgG that develops during natural infection correlates with severity rather than protection”.
Briefly, Shrock E et al (Science, 2020) reported that a stronger and broader antibody response to SARS-CoV-2 peptide antigens correlated with severity which they found counterintuitive. Lucas C et al (Nature Medicine, 2021) reported that levels of anti-Spike correlated with severity and that the deceased had higher levels of anti-spike antibodies than those who were discharged.
Legros V et al (Cell Mol Immunol, Feb 2021) reported that the levels of neutralizing antibody (NAbs) correlated with severity, whereas those with asymptomatic infections had low or no NAbs. Finally, Woodruff MC et al (Nature Immunol, 2020) showed that the early production of NAbs was associated with more severe disease and that NAbs (around 1/1000 dilution) that occurred during the day 5 to 15 window were associated with a higher risk of death.
This means, as expected for an emerging RNA virus that the host has never seen before, the host must rely on innate immune mechanisms for protection against pandemic viruses.
Indeed, over the past few million years, human evolution has by necessity, focused on strengthening innate immune mechanisms. Perhaps about 800,000 years ago humans acquired a “virus anti-virus system” called human endogenous retrovirus K102 (HERV-K102) which is detailed elsewhere (hervk102@substack.com). Suffice it to say, when these protector foamy virus particles are induced in M1-like macrophages it renders the macrophages foamy. On day 6 these protector particles are released by cell lysis. Of relevance to protection against an emerging pandemic respiratory RNA virus, sebocytes in sebaceous glands that line various mucosal tissues such as in the nasopharyngeal-oral mucosa, are specialized foamy macrophages constitutively producing and releasing protector HERV-K102 particles by lysis. This waxy substance largely consisting of HERV-K102 particles is known as sebum. In addition to the particles being protective by undergoing lytic infections in virus infected cells, upon their release, they trigger the activation and release of antibody to HERV-K102 envelope from innate B cells. HERV-K102 envelope is expressed on tumors and virally infected cells but not on normal cells. So this autoantigen serves as a means for clearance of virally infected cells. Also for enveloped viruses like SARS-CoV-2, as it buds from the cell surface its particles pick up HERV-K102 envelope. Accordingly, the HERV-K102 antibodies can also clear and/or inactivate SARS-CoV-2 virus particles. So if the host innate immunity can clear the pandemic RNA viral infection say by the first 10 days, then there are no worries about developing the ‘neutralizing antibodies’ of adaptive immunity and the complications it can bring.
This scenario of what happens at the host level is recapitulated at the population level. First, the exaggerated levels of IgG neutralizing antibodies induced by the administration of the second dose of mRNA vaccine will quickly select for immune escape mutant strains (see previous posts at hervk102@substack.com). Achieving ‘herd immunity’ becomes more impossible with time. We see for example how the 2 dose mRNA vaccines loose vaccine effectiveness against symptomatic infection (> 6 days after the 2nd dose is administered) whereas boosted trained innate immunity (< 7 days after the second dose of the mRNA vaccines are administered) achieves and then maintains sterilizing immunity throughout the rest of the pandemic irrespective of the variant (Figure 1 compiled from Tartof SY et al., Lancet October 4, 2021).
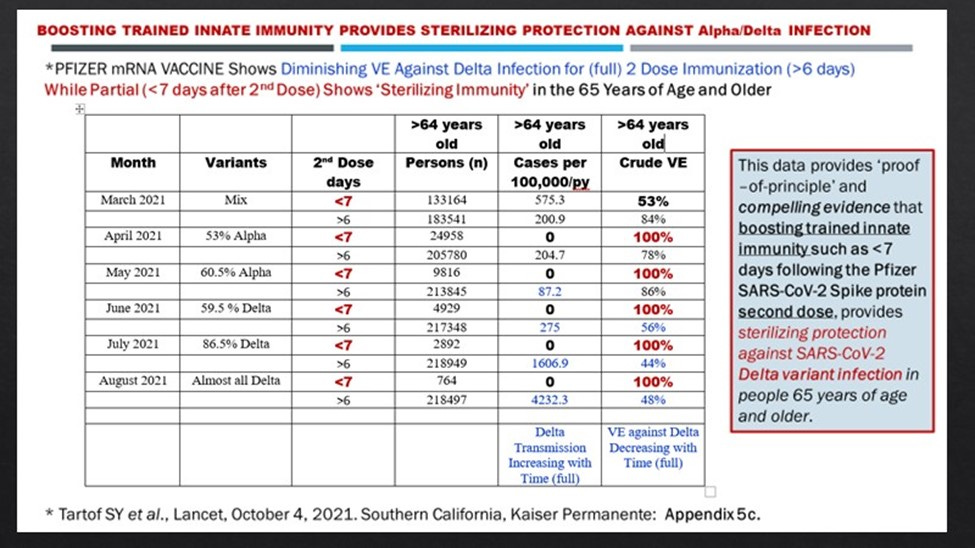
Figure 1. Loss of vaccine effectiveness (VE) against symptomatic infection gets worse with time with adaptive immunity vaccination whereas boosting trained innate immunity provides sterilizing immunity needed to establish herd immunity.
My Efforts to Warn About Not Using Adaptive Immunity Vaccines against an RNA Virus Pandemic
Suspecting that public health authorities may attempt to make adaptive immunity vaccines against a pandemic RNA virus which could prove disasterous, I swiftly acted in early 2020 to contact the relevant health authorities to urgently request that they investigate if HERV-K102 particles protect against COVID-19 infection and/or help mediate recovery. If so, then adaptive immunity vaccines would clearly be contraindicated.
As Research Manager of the Blood Zoonotics Unit in the Blood Safety Program at the Public Health Agency of Canada (PHAC: 2000 - 2011), I had worked directly under Dr. Howard Njoo towards the end and knew well the efforts at that time by Dr. Theresa Tam to organize ‘pandemic preparedness strategies against influenza’. Dr. Njoo is now the Assistant Chief Public Health Officer (CPHO) and Dr. Tam the CPHO. I contacted them early in 2020 to indicate that they would need to study the trained innate immunity in COVID-19 patients afforded by HERV-K102 particle production to verify that innate immunity rather than adaptive immunity provided protection against and recovery from COVID-19. I knew that addressing this issue early was important, as it would impact whether adaptive or innate immunity vaccines (if any), should be the strategy of choice to end the pandemic.
I reminded them of my PHAC work which had implied HERV-K102 particle activity was associated with resistance to HIV-1 acquisition (sterilizing immunity) in a “seronegative cohort” arranged through the late Dr. Frank Plummer (who I had the pleasure of working directly under temporarily in the summer of 2006 at the Centre for Infectious Disease Prevention and Control when my supervisor Dr. Tony Giulivi was unexpectedly dismissed). It was well established and still true that adaptive immunity vaccines against HIV-1, another pandemic RNA virus, did not work and in some instances led to enhanced infection. For the latter reason, I was a voluntary working group member of the Brighton Collaboration for the Viral Vectored Vaccine SAFETY Working Group (2008 - 2015) which was run by Dr. Robert Chen.
I even wrote an article on clues that reveal it is the innate immunity HERV-K102 protection system which may be a correlate of risk/protection against HIV-1 in order to explain how adaptive immunity vaccines do not block acquisition of HIV-1. This paper has been viewed over 900 times and is highly recommended.
“Laderoute M. Clues to finding correlates of risk/protection for HIV-1 vaccines. F1000 Research 2018, 6:868. https://doi.org/10.12688/f1000research.11818.2”
Clearly Dr. Frank Plummer at the time as the Scientific Director General of the National Microbiology Laboratory at PHAC and Dr. David Butler-Jones, the first CPHO of Canada and head of PHAC, knew my scientific discovery was important, as they arranged for international patent applications (since abandoned upon their respective retirements from PHAC). Upon Dr. Butler-Jones’ retirement, the Harper government set up a parallel structure to govern PHAC, where non-medical and non-scientific personnel would control the shots (literally and figuratively), and thus any outcome of pandemics. I think we can see now why this may not have been such a good idea.
In addition to attempting to get PHAC to perform the necessary scientific investigation to determine if HERV-K102 would provide “protective immunity against an emerging pandemic RNA virus, SARS-CoV-2” (as was found for HIV-1), I also contacted Dr. H. Clifford Lane who is the NIAID Deputy Director for Clinical Research and Special Projects at the NIH. This office co-ordinates intramural and extramural research involving human volunteers. I sent the methods for monitoring HERV-K102 particle production and for antibody to HERV-K102 envelope but again to no avail. I also sent similar warnings to the CDC and the WHO also without any response.
Others Warned Against Adaptive Immunity Vaccines Due to ADE
In addition to the two Belgian scientists who were very vocal on social media, other scientists also got a chance before censorship to warn about the dangers of antibody dependent enhancement of infection (ADE). These included: the Lee et al (2020) group mentioned above, and the following papers: Wen J et al, Int J Inf Diseases Nov 2020; Arvin AM et al, Nature, August 2020; and Karthik K et al., Hum Vaccin Immunotherapy, Dec 2020. As well, the concern that rushing the randomized clinical trials (RCTs) and approvals of these vaccines could not possibly provide a reasonable measure of safety was raised in 2020 (Khuroo MS et al., J Clin Exp Hepatol, June 2020). Another issue raised was that the informed consent forms for the RCTs did not alert the volunteer to the real risk of ADE and enhanced death possibilities as noted by Cardozo T & Veazey R (Int J Clin Pract, March 2021).
And so today we do have evidence that human macrophages ARE infected by SARS-CoV-2 in vivo but only as associated with ADE in those with severe COVID-19 (Ren X et al, Cell, 2021). As assessed in a human macrophage model, these ADE antibodies were commonly detected in elderly patients who experienced more severe COVID-19 (as detected in convalescent plasma). Moreover this infection of macrophages in vitro does lead to upregulated release of IL-6 at 3 days (Shimizu J et al., Sci Reports, 2021) and where IL-6 levels in the blood is well established to be associated with increased risk of COVID-19 morbidity and mortality. In addition both positive and negative strands of SARS-CoV-2 RNA were demonstrated in the macrophages in bronchoalveolar lavage fluids (BALF) from severe patients by Ren X et al., (Cell 2021). This implied SARS-CoV-2 was actively replicating in these macrophages. Other research groups had previously shown the replication of SARS-CoV-2 in macrophages in vivo in BALF from patients with severe COVID-19 (reviewed by Ren et al.). Thus, we can expect neutralizing antibodies induced by vaccination are likely to be harmful for the host and at the population level, to select for more transmissible and more pathogenic variants exacerbating the pandemic.
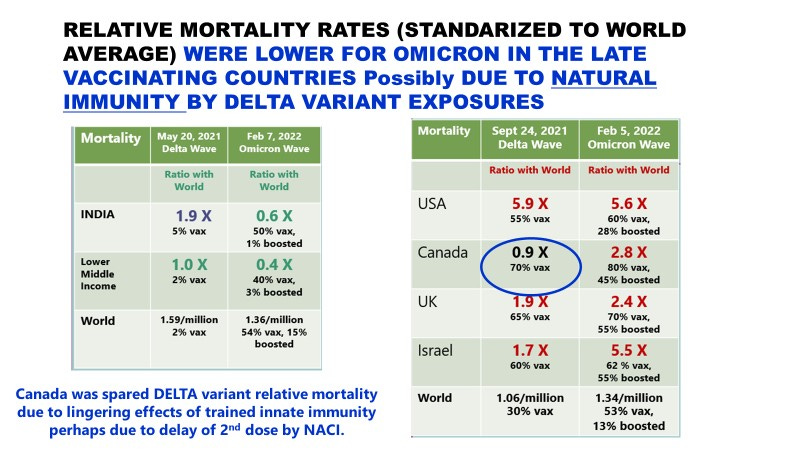
To reiterate, herd immunity to an emerging RNA virus cannot be achieved by adaptive immunity vaccines. Accordingly, the notion that mandating adaptive immunity vaccines would help in any way to increase herd immunity and help end the pandemic is a complete fallacy. In fact, the opposite is true. Through the selection of variants, there will be successive waves of more transmissible and generally more pathogenic variants. [Note it appears omicron may have been derived from or evolved in the common house mouse (no adaptive immunity vaccines) and while is regarded as less pathogenic than delta its increased transmission (related in part to ADE) may have caused more mortality per million than delta. See numbers in the attached powerpoint below.]
New Evidence Consistent with HERV-K102 Particles and Antibody Being Protective Against COVID-19
In the end, while no one ever tested specifically for HERV-K102 particles or HERV-K102 envelope specific antibodies in COVID-19 patients, I did recently stumble upon some data consistent with an upregulation of HERV-K102 particles with severity potentially as may be needed for recovery from the harms of SARS-CoV-2 specific neutralizing antibodies. This data from Maugeri N et al ( J Thrombosis and Haemostasis, 16 May 2021) suggests that ITGB3+, HMGB1 + extracellular vesicles (EVs) of about 120 nm correlate with COVID-19 severity (Figure 2). This includes correlations with C-reactive protein (CRP), D dimer, poor oxygen saturation, lactate dehydrogenase, acute respiratory distress syndrome (ARDS) and the WHO score for clinical deterioration. Since there were 23 deaths of 97 hospitalized patients, this suggests these particles could have been associated with the 76% survival rate although oddly, there was no analysis of outcome in terms of absence of particle levels and risk of death. It seems the authors were intent on showing how harmful these particles were. I suspect they did do the calculations but since it didn’t fit their narrative, they just ignored the data. On the other hand, in those with sepsis, it is known the elevated particles persist after recovery, indicating they were likely part of the recovery (Wang G et al., Cell Death Discovery, November 2021).
Wang G et al (2021) have shown that in sepsis it is the macrophages that generate these particles in humans and that transferrin on the EVs mediates their uptake in the liver as tested in mice, where they mediate pyroptosis (fast cell death) by activating the NLRP3 inflammasome. Of relevance to HERV-K102 particles, in addition to the tetraspanins CD63, CD9, and CD81, these sepsis associated EVs carry not only HMGB1, RAGE, EEA1, rab5, rab7, and transferrin but they carry Lamp1. Lamp1 is the cytoplasmic signalling molecule for the cytoplasm generated DNase-2 dependent mode of programmed cell death used for the holocrine secretion of sebum (foamy sebocyte apoptosis) [Fischer H et al., J Invest Derm, 2017]. Very likely Lamp1 is also used for the day 6 apoptosis of foamy macrophages needed for the release of the HERV-K102 particles. Thus, indirectly this provides further evidence consistent with the notion that HERV-K102 particles may rapidly induce lysis in virus infected cells (within 24 hours, see data in a previous post at hervk102@substack.com). On the other hand, in normal cells, HERV-K102 simply integrates into the genomic DNA increasing the proviral copy number. This was shown for the HIV-1 exposed seronegative (HESN) cohort resistant to HIV-1 acquisition and thus, was associated with sterilizing immunity (Laderoute M et al., Open AIDS J, 2015).
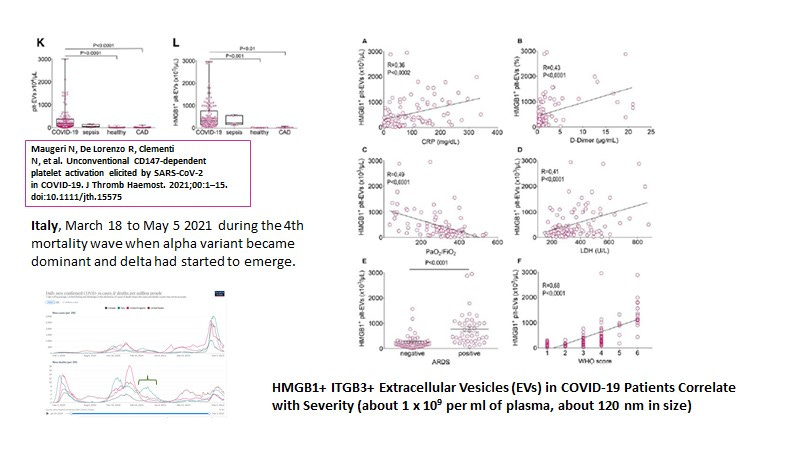
Figure 2. HMGB1+ ITGB3+ Extracellular Vesicles Correlate with COVID-19 Severity
In another instance, and interestingly, involving the same clinical trial cohort, the San Raffaele hospital COVID-19 cohort in Italy, they observed that “neutralizing antibodies” present in the first 2 weeks and up to 4 weeks correlated with with a faster clearance of SARS-CoV-2 in the nasopharyngeal swabs (NPS). Moreover they suggested that the absence of these “neutralizing antibodies” placed the host at a higher risk of death (Figure 3).
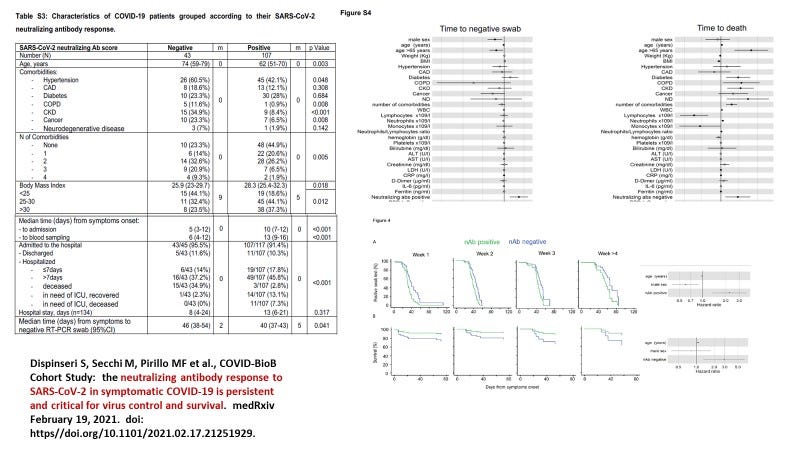
Figure 3. Neutralizing Antibodies in the First 4 weeks after Onset of Symptoms Result in Faster Clearance of SARS-CoV-2 in NPS and Their Absence Correlated with Increased Risk of Death (Dispinseri et al., 2021). Note the inverse correlation of benefit with age probably reflecting how immunosenescence interferes with HERV-K102 particle release from foamy sebocytes (NPS) and foamy macrophages in the lungs.
Please note this article has been published in Nature Communications:
Dispinseri S, Secchi M, Pirillo MF, Tolazzi M, Borghi M, Brigatti C, De Angelis ML, Baratella M, Bazzigaluppi E, Venturi G, Sironi F, Canitano A, Marzinotto I, Tresoldi C, Ciceri F, Piemonti L, Negri D, Cara A, Lampasona V, Scarlatti G. Neutralizing antibody responses to SARS-CoV-2 in symptomatic COVID-19 is persistent and critical for survival. Nat Commun. 2021 May 11;12(1):2670. doi: 10.1038/s41467-021-22958-8.
However, as I mentioned above, the adaptive immune system is too slow and doesn’t even produce antibody of any significance until well after 2 weeks. Indeed if we look at the numbers we see there were no significant levels of spike specific antibody before 5 weeks in the study (Figure 4) indicating these “neutralizing antibodies” were not part of adaptive immunity. Others have similarly reported that the mean and median onset of neutralizing antibodies to SARS-CoV-2 in the ‘naive’ naturally infected is 5 weeks after onset of symptoms whereas for the two dose vaccinated, it takes a mean of 10 weeks and a median of 15 weeks after the first dose (Hofmann N et al., Sci Reports, 2022).
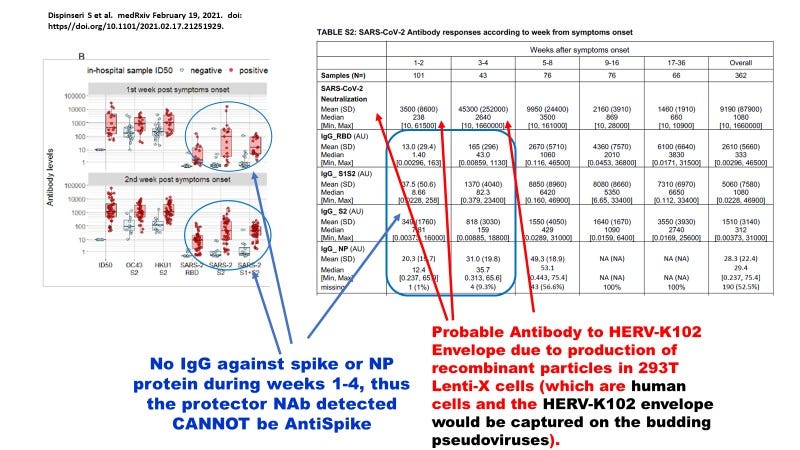
Figure 4. The “Neutralizing Antibodies (Dispinseri et al., Nature Communications, May 2021)” are not against spike protein and most likely are Innate Antibodies to HERV-K102 Envelope and/or Possibly HERV-K102 Particles Released on Day 6 from Sebocytes and Foamy Macrophages
Instead the early onset implies that these are innate immunity antibodies, and very likely the antibodies to HERV-K102 envelope. This error was caused by producing the pseudoparticles for the neutralizing antibody test in human rather than the typical primate VeroE6 green monkey cells. The preparation of particles for neutralizing antibody assays in human cells are going to pick up HERV-K102 envelope in the pseudoparticles as they bud through the cell surface. Here they used the Lenti-X human embryonic kidney 293T cell line to create the particles. In the two papers quoted above (Legros et al, 2021 and Woodruff et al, 2020) they used SARS-CoV-2 propagated in the VEROE6 line and thus, were not subject to this interference for the interpretation of NAbs.
There have been lots of modifications to the gold standard Plaque Reduction Neutralization Test (PRNT) which in its original format required the use of a BL3 lab to culture SARS-CoV-2 in VEROE6 cells and then to perform the testing for neutralization of SARS-CoV-2 entry and replication on an indicator cell line usually VEROE6 (Kay GA et al, Sci Rep, March 1 2022). Indeed, Savage et al (Savage HR et al., PLoS Negl Trop Diseases, July 8, 2021) have remarked that surprisingly, the correlation of SARS-COV-2 IgG with the presence of neutralizing antibodies was low with some of these other modified tests, whereas in all cases there was a strong correlation of IgG levels with COVID-19 severity (r value of 0.756). Moreover, those papers using the pseudovirus methods for virus neutralization showed the highest incidence of the presence of neutralizing antibodies to SARS-CoV-2 while those using SARS-CoV-2 propagated in VEROE6 cells, showed the least.
Accordingly, these authors have misrepresented the real protection by innate immunity (HERV-K102 antibodies as likely would be found in early plasma samples from 1 to 4 weeks) as “neutralizing antibodies to SARS-CoV-2 spike protein.”
So in conclusion, while we still need to URGENTLY directly test for HERV-K102 particles and antibody to HERV-K102 envelope in COVID-19 patients, taken altogether it appears that the HERV-K102 innate protector system and not the SARS-specific neutralizing antibodies which protect against death.
Given the explicit understanding developed here that adaptive immunity cannot stop a pandemic and can make the death toll worse, the question remains as to whether we can explain why omicron which was supposed to be far less pathogenic than delta, seemed to cause much more death in Canada, the US, the UK and Israel than anticipated.