

What might excess all cause mortality rates tell us about the emergence of SARS-COV-2 variants, and overall effects of vaccines on mortality during the pandemic in Canada?
What might excess all cause mortality rates tell us about the emergence of SARS-COV-2 variants, and overall effects of vaccines on mortality during the pandemic in Canada?
February 22, 2022 Final Version


Summary Slide:
Key Inflection Points in the EACM Profile with Time And Emergence of the Alpha (Yellow) and Delta (Pink) Variants; Layered Over COVID-19 Mortality Per Million with Time (Faint Lavender) for CANADA
Abstract: The appropriateness and safety of using an adaptive immunity vaccine (two doses of mRNA) to control an emerging RNA pandemic RNA virus was questioned due to the anticipated: antibody dependent enhancement (ADE) of infection and pathogenesis, the potential for the selection of variants (by ADE), the inability to reach herd immunity (due to ADE), and the potential perpetuation of the pandemic with new waves of variants of concern. Using various data available at Our World in Data, the goal was to test the hypothesis that selection for the alpha and delta variants occurred with adaptive immunity vaccination (2 doses of mRNA vaccine) but not with innate immunity vaccination (1 dose of mRNA vaccine) in Canada. The percentage vaccinated (totals, two dose and one dose) and a ratio of two dose per one dose were tabulated for the weeks from December 22, 2020 through August 1, 2021 which covered the emergence and dominance of the alpha and delta variants in Canada. The COVID-19 mortality per million plot was examined and layered under the excess all cause mortality plots (% excess deaths over the previous 5 years). The latter showed a period of negative excess all cause mortality from February 10 to April 28, 2021 with the apex of the trough (maximal heterologous or non-specific protection associated with one dose of vaccine) at March 21, 2021. The emergence and then dominance of the alpha and delta variants occurred either when the two dose to one dose ratio exceeded 0.50 (alpha emergence and delta dominance) or when the heterologous protection of one dose significantly dropped (alpha dominance and delta emergence) as demonstrated by significant inflection points in the excess all cause mortality plot. It is suggested the adaptive immunity vaccination (two doses of the mRNA COVID-19 vaccines) selected for variants through ADE mechanisms at the level of macrophages which was concomitantly associated with the loss of heterologous protection of trained innate immunity at the level of macrophages. In conclusion, a two dose adaptive immunity approach failed to stop the pandemic in Canada due to selection of variants. Adaptive immunity vaccines are not an optimal approach to controlling pandemic RNA viruses.
Introduction
There was a remarkably rapid advent of COVID-19 mRNA vaccines at the start of 2021 available through emergency use authorization (EUA). In 2020, before these vaccines suddenly appeared there was open and unimpeded discourse by clinicians, medical scientists, immunologists and vaccinologists about the concern of antibody dependent enhancement (ADE) for any type of vaccine against SARS-CoV-2. The reason was that it was well-known that vaccines against emerging RNA viruses with pandemic potential (meaning they cause significant morbidity or mortality), due to their recent transmission to humans (usually from another species), were not safe. The fact that vaccines have not been produced against another significant and current pandemic RNA virus, HIV-1 which emerged around 1983 (almost 40 years ago), is a case in point. It was not due to a lack of funding nor a lack of trying. It has been almost 20 years since the SARS pandemic, and still no safe vaccine for coronaviruses.
RNA viruses mutate quickly when compared with DNA viruses as they carry less mutation correction mechanisms. This means once inside the host, instead of a single virus, there is a swarm of mutated viruses called viral quasispecies that rapidly develop. Any attempts by spike specific antibodies (ie., adaptive immunity ones) to stop the initial or wild type strain from replicating is simply met with the emergence of ‘immune escape mutants’ which have been selected for by the antibodies. If you consider the fact that it takes adaptive immunity a full two weeks to generate a response against a novel virus that it has never seen before, highly pathogenic emerging viruses would kill you long before then. In fact, after the first two weeks, adaptive immunity antibodies play catch up with the virus. By the time the antibodies initially develop, immune escape mutants have already emerged and this cycle simply repeats itself, more or less like a ‘do loop’. So the antibody arm of adaptive immunity is simply not well suited to handling pandemic RNA viruses. Hence, in the last few million years of Homo sapien evolution there has been selection for improvements to innate immune mechanisms against emerging RNA viruses. A critical one of these concerns the acquisition by humans of a virus anti-virus response called human endogenous retrovirus K102 (HERV-K102) which you can read about in my previous blogs.
As the great vaccinologist, Dr. Geert Vanden Bossche would gladly tell you, the problem with adaptive immunity vaccines which generate antibodies near or at the receptor binding domain of the virus (here spike protein) along with neutralizing antibodies, is that they rapidly select for variants which prolongs the pandemic. Even worse, through ADE mechanisms this targets the virus to macrophages through Fc receptors (receptors for the neutralizing antibodies). Since this knocks out innate immunity, now ADE promotes enhanced virus infection, transmission and replication. Depending on what other cells the virus targets, uncontrolled replication can lead to enhanced pathogenesis. Generally for emerging RNA viruses there is an evolution towards increased infectivity and transmission with time, but reduced pathogenesis. However, if there is selection by antibodies the virus will mutate for enhanced pathogenesis (Lythgoe KA et al., Evolution, 2013). ADE easily explains the former and the latter since it targets the main cell type of ‘trained innate immunity’ the foamy macrophages in tissues and sebocytes in the mucosa (Slide 1). The more ADE the less trained innate immunity to clear the infection thus transmission and infection rates rise. The less the trained innate immunity the poorer the defense and the higher likelihood for increased replication and associated pathogenesis.
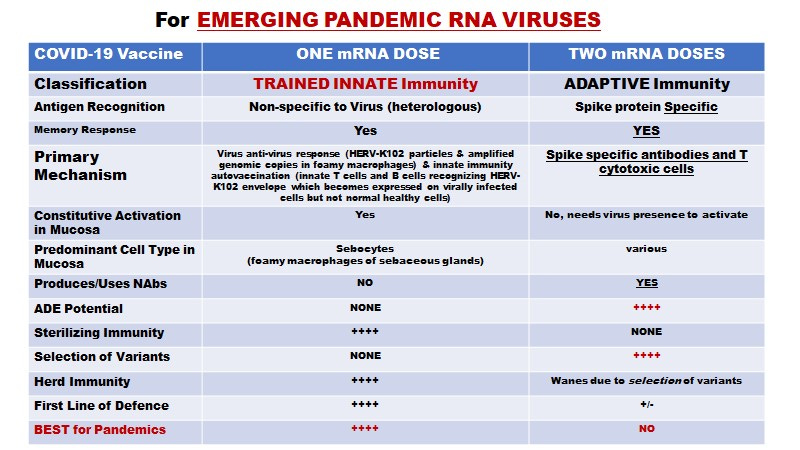
NAbs = neutralizing antibodies
Slide 1. Important Differences Between Trained Innate and Adaptive Immunity
Note that constitutive activation in mucosa for Trained Innate Immunity only refers to the production and lytic release of HERV-K102 particles from the foamy macrophages (called sebocytes) in sebaceous glands. The autovaccination process which generates innate T cells and IgG2 antibody to HERV-K102 envelope occurs in the periphery in response to viral infection of monocytes/macrophages.
As Lee SL et al. (2020) aptly pointed out, you know you are going to have a problem with ADE with a virus when seroconversion and the development of neutralizing antibodies correlate with clinical severity rather than protection as was observed for SARS-CoV-1 and now SARS-CoV-2 (Chvatal-Medina M, et al., Front Immunol April 2021). This correlation was well established early in the pandemic. Older patients (who are at increased risk of immunosenescence which results in failed trained innate immunity) are more likely to develop ADE (Shimizu J et al., Science Reports December 2021). It is noteworthy that the model used by Shimizu et al., concerned real ADE as measured directly on human macrophages under conditions that favor and do not block trained innate immunity involving HERV-K102 (i.e., they did NOT use RPMI media which blocks HERV-K102 particle production in macrophages). For the first time, it was demonstrated that ADE enhanced IL-6 activity after 3 days. This was extremely important as IL-6 activity correlates clinically with COVID-19 severity. Indeed, Jensen B et al., (The Lancet Regional Health, July 2021) documented how in vivo treatment of severe (older and immunocompromised) COVID-19 patients with a neutralizing monoclonal antibody selects for escape mutants which emerge and dominate on average by a mere 10 days.
So given the historical expectation that a safe vaccine against an RNA pandemic RNA virus would be unlikely, it was quite surprising to most knowledgeable persons, that a) any COVID-19 vaccine would get an EUA, b) that public health authorities would encourage their use, and c) that early treatment (the test and treat strategy for example, involving ivermectin and/or hydroxychloroquine) was not only ignored but actively suppressed. The EUAs were based on data that showed that 2 doses of the vaccine (encoding wild type spike protein) provided 90% or better vaccine efficacy (VE) against symptomatic infection but as studied for only two months during which the wild type virus predominated. Since the point of vaccination is to protect the most vulnerable from severe disease and death, it is noteworthy that no clinical trial data supporting this was submitted for EUA or even subsequent vaccine approval. No vaccine efficacy against expected variants were studied and worse, the longer term safety assessment (usually around 2-5 years) was curtailed early (2 months) due to evidence of 90 % or better VE against symptomatic infection and the trials were stopped.
It is noteworthy that a massive censorship of all the discourse on the subject of COVID-19 vaccine safety and efficacy as well as alternative treatments such as involving ivermectin and/or hydroxychloroquine, was promulgated by public health authorities and government. Worse, and probably to stoke the fearmongering tactic as well as encourage compliance, public health authorities and governments introduced vaccine mandates which simply put, are unconstitutional for democratic societies.
So a number of important questions arise. First, during emergence of variants of concern, is a person over the age of 59 who receives the two dose COVID-19 vaccine at higher risk of symptomatic infection than someone naturally infected? Second, did the use of the 2 dose vaccine in the over 59 years of age select for variants of concern in Canada? Third, how did vaccination impact excess all cause mortality (ACM) in Canada?
Results
Two Dose Vaccination Not Very Protective Over Natural Immunity in the 60 Years of Age and Older During the Alpha and Delta Waves in Israel
In Slide 2 are presented the OR data on symptomatic breakthrough infections in the doubly vaccinated versus reinfections in the unvaccinated but previously infected cases (Table 2b from Gazit S et al., medRxiv August 25, 2021), and covers the time when alpha was dominant in Israel (>80% prevalence of the alpha variant from February 22, 2021 to May 31, 2021). It also covered the time of the emergence of the delta variant (>50 % prevalence from June 14 onwards although the data was followed only to August 14th. The OR of 27 (p<0.001) (95 CI of 12.7 to 57.5) is remarkable for increased risk of symptomatic breakthrough infection associated with 2 doses of vaccines for matched dates of events (Table 2b) when compared with reinfection rates in the naturally infected. When stratified by age >59 and compared with the age group 16-39, the odds ratio was 2.89 (95 % CI of 1.68-4.99, p<0.001) consistent with the risk of ADE in promoting infection which may be more prevalent in those 60 years of age and older.
The absolute increased risk of breakthrough infection in the doubly vaccinated over the previously infected (all ages and where the mean age for this study was 36 years of age) was 1/84 in this study albeit, during a time when either or both SARS-CoV-2 variants were circulating/evolving. However this is concerning as it represents a common serious adverse effect of vaccination (ie., vaccine failure and ADE) for the general population. Since 69 % of all breakthrough infections occur in the >64 years of age [https://www.kff.org/coronavirus-covid-19/press-release/breakthrough-covid-19-hospitalizations-among-fully-vaccinated-patients-occur-most-often-among-older-adults-and-involve-people-with-chronic-health-conditions/] but only 5 % of the participants in this study were over the age of 59, one can roughly guesstimate that for the over 59 years of age, the risk is higher, possibly up to about 1/10.
With regard to pathogenesis, while there were no deaths in this Israel study, as shown in Slide 2, there were 8 people hospitalized in the doubly vaccinated group and only one in the previously infected, unvaccinated. The OR for hospitalization was 8.06 (95% CI 1.01-64.55) with a p value of 0.049. However the age stratification analysis for the comparison of the over 59 to the 16-39 age group revealed fully vaccinated people >59 years of age were about 161 times more likely to be hospitalized if they experienced a breakthrough infection (OR 160.9 (95% CI 19.91-1300.44, p<0.001) than those who were not vaccinated but previously infected and re-infected.
The impact of boosting trained innate immunity with one dose of mRNA vaccine was studied by Gazit et al., 2021 again in a population where the mean age was 36. The comparison of OR for the previously infected with and without one dose of vaccination (Slide 2, Table 4a) the OR of 0.53 (95 % CI 0.30 - 0.92, P=0.023) showed enhanced protection against reinfection in the previously infected with one dose of vaccine. This showed boosting innate immunity enhanced protection. However, curiously, no comparisons were made of previously infected with one dose of the COVID-19 vaccine with two doses.
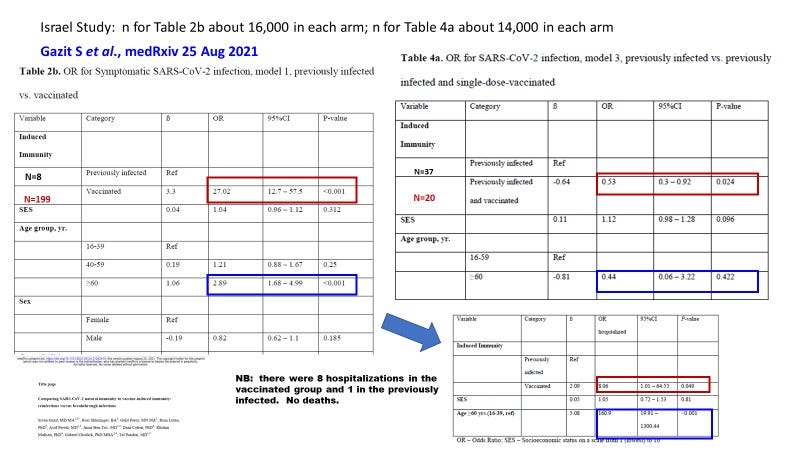
Slide 2. For symptomatic breakthrough or reinfection, 2 dose vaccination may be associated with up to a 27 fold increased OR of breakthrough over reinfection, and is exacerbated by age >59. In contras, one dose vaccination in the previously infected reduces risk of reinfection over those previously infected (but not vaccinated) (see Gazit S et al., medRxiv, August 25, 2021).
Important Differences Between One Dose and Two Doses of COVID-19 Vaccines
In order to understand the data about to be discussed, the reader must understand that one dose mRNA vaccination triggers innate immunity while two mRNA doses triggers adaptive immunity, including heightened levels of spike specific antibodies and the neutralizing antibodies (Slide 1). It is the latter which strongly selects for variants.
Canadian Mortality DATA During the Pandemic
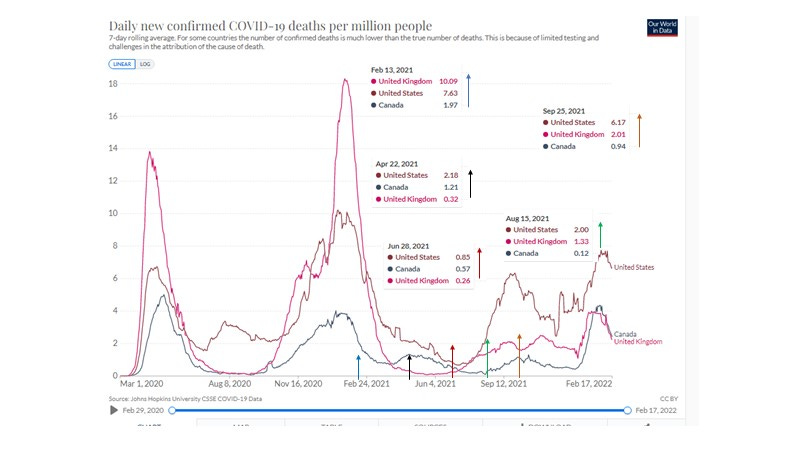
Slide 3. 7 day Moving Average COVID-19 Deaths per Million Comparing Canada with the UK and the USA
One of the most useful parameters used to study mortality risks due to pandemics would be the actual 7 day moving average of deaths per million coded to COVID-19 shown in Slide 3 for the USA, the UK and Canada. By reporting deaths per million (population) this allows for a direct comparison of the burden of death by country. Briefly, Canada suffered the lease in terms of per capita mortality to COVID-19 and exhibited 5 waves: wave 1 wild type; wave 2 wild type; wave 3 alpha; wave 4 delta and wave 5 omicron (Slide 4). The UK did not have wave 3 because alpha was already dominant in the second wave (which was the biggest wave for the UK). The August 8, 2020 summer wave in the USA pertained to the southern states which were largely not affected in the April-May 2020 wave which instead affected the north-east states and Washington State.

Slide 4. COVID-19 mortality per million in Canada
July 19, 2021 refers to a point in time when about 50% of the Canadian population was fully vaccinated.
EACM (Excess All Cause Mortality)
The most useful parameter for examining mortality is excess all cause mortality (EACM) (Slide 5) which is not subject to biases in labelling the cause of death (Corrao G et al., J Hypertension, May 2021). Unlike problems or changes in testing for cases which affects the case fatality rates, EACM is perhaps the most reliable. It plots the excesses in deaths (7 day moving average) over the 5 previous years expressed as a percentage and allows for direct comparisons to other countries. Importantly it has the power not only to examine the impact of COVID-19 deaths directly but may also give valuable information on the indirect effects of the pandemic or vaccination etc. on deaths. This might include deaths associated with chronic diseases and other causes. For example, in the USA the fear and anxiety from the fearmongering, lockdowns, loss of jobs, reduced income, reduced schooling, limitations on socializing, banned travel to see family members, etc., appears to have lead to a persistent 10% excess all cause mortality at least in 2020 (Fairman KA et al., BMJ Open, 2021 and Glei DA. medRxiv, October 23, 2021) but as expected also for 2021.
Canada experienced a major peak of excess all cause mortality during the first wave, and a sudden sharp peak on July 4, 2021 (Slide 5). This peak reflected 1077 excess all-cause mortality deaths which involved only 264 COVID-19 deaths and 526 heat-related deaths from British Columbia. This is why it was not seen in other countries.
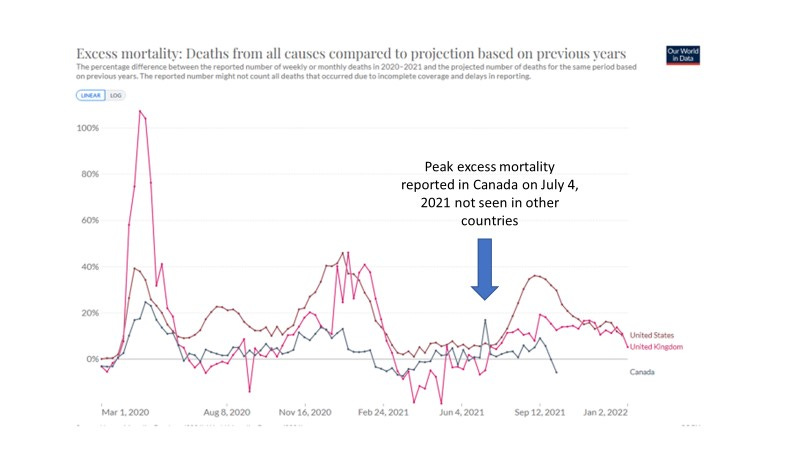
Slide 5. Excess Mortality in Canada March 1, 2020 to Late September 2021.
In Slide 6, we clearly see a sustained period of negative excess all cause mortality (ACM) (February 10 to April 28, 2021) when compared with all cause mortality of previous years. As mentioned the July 4 2021 peak is not relevant.
Behind the EACM profile, I have added the COVID-19 mortality per million profile (faint grey) for reference. We can see that there is a significant drop in EACM from January 3, 2021 to about April 28, 2021 while the COVID-19 specific deaths were occurring. From January 3 to February 10 this was associated with a positive EACM value (net excess mortality) involving the period of vaccination in about 38 % of the 80+; while from February 10 to April 28 this was associated with a negative EACM value (net protection against mortality) involving the period where the remainder of the 80+ and all the 60+ plus an additional 40% of the 55-59 years of age were immunized.
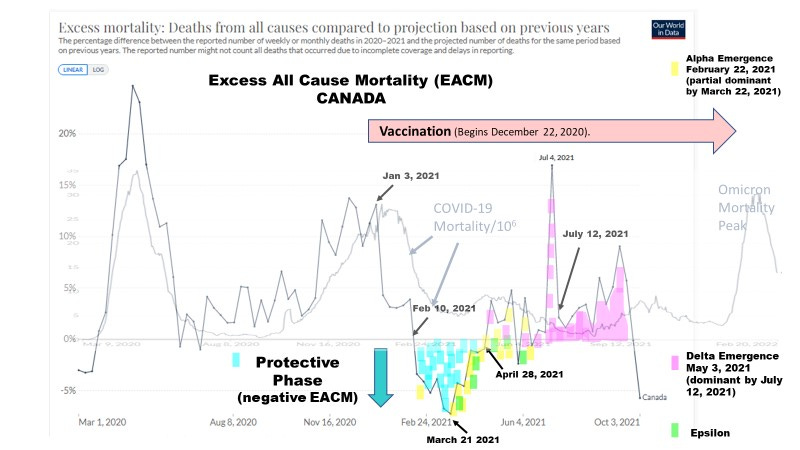
Slide 6. A Sustained Negative Excess All Cause Mortality in Canada Around the time of Vaccination.
Historically, 56% of the total EACM for March - December 2020 was in the 75 years of age and older and another 20% in the 65 - 74 age group (USA excess ACM statistics: Glei DA. medRxiv October 23, 2021).
Therefore to study the effects of vaccination on a) emergence of the alpha variant (first detected February 22, 2021 at 14 %, first dominant March 22 at 44 %) and the delta variant (first detected May 3, 2021 at 1%, first dominant July 12 at 52%) and b) on the negative EACM, partial and full vaccination was highlighted in these age groups.
In Canada, as in other countries, vaccine rollout was by descending age (Slide 7).
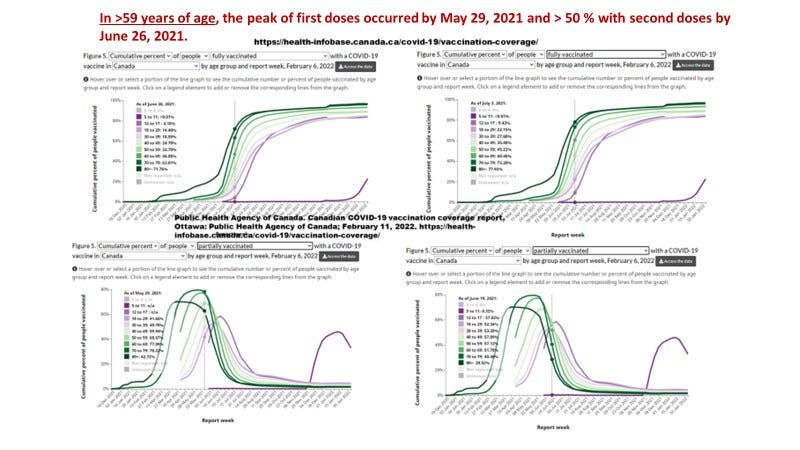
Slide 7. Vaccination Rollout by Descending Age in Canada
In Slide 8 are given the % of the Canadian population given at least one dose (provides the actual % of the population vaccinated), the % with 2 doses, the % with one dose and the Two Dose to One Dose Ratio. For convenience it summarizes the findings on variant selection (under events) and under Notes for EACM.
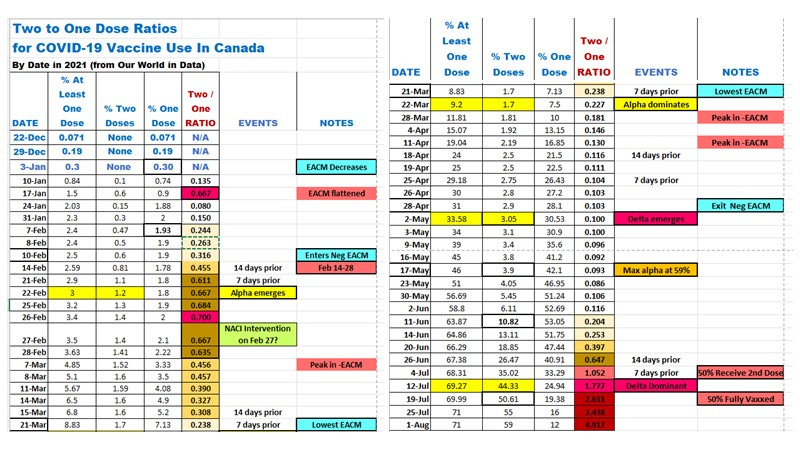
Slide 8. Vaccination by Partial/Full and Impact on EACM and SARS-CoV-2 Variant Selection by DATE (sourced from Our World in Data)
Variant Selection in Canada
On January 4, 2021 SARS-CoV-2 was 98% wild type and no previous evidence of the alpha or delta variants.
The Alpha Variant Emergence in Canada (Feb 22, 2021)
Fully vaccinated individuals were reported on February 13, 2021 at 1.55% for the 80+ and 0.31% for the 70-79 age category representing about 55,777 persons. No person at any other age had received 2 doses by this time. In Slide 8, we see the emergence of alpha associated with an elevated two/one dose ratio of about 0.455 about 2 weeks prior implying the possibility of ADE contributing to the alpha variant emergence on February 22, 2021. Congregation at vaccine centres may have increased the likelihood of transmission/infection especially because these age groups being vaccinated at this time represented a gathering of the most vulnerable.
The Alpha Variant Dominance in Canada (March 22, 2021).
On March 22, 2021, 8% of the 80+ and 2% of the 70-79 age group were fully vaccinated. Again no other age group received two doses. This represents 302,360 people who had received 2 doses of the vaccine approximately on March 8, 2021. The dominance of alpha likely pertained to a persistently high two/one dose ratio from about Feb 14, 2021 to March 15, 2021 (Slide 8).
While the alpha variant could have also evolved in unvaccinated but severely infected recovered or expired Canadian patients, and/or could have been imported, it is noteworthy that the alpha variant gained a foothold in Canada subsequent to the initiation of 2 doses of vaccine in the most vulnerable, meaning that a contribution cannot be formally ruled out.
The Delta Variant Emergence in Canada (May 3, 2021)
On April 24, 16 % of the 80+ group, 5% of the 70-79 age group, and 2 % of the age 60 to 69 age group were fully vaccinated for a total of 732,940 persons. In addition 3% of the age 50-59, 3% of the age 40-49, 2% of the 30-39 age group and 2% of the 18-29 had received the second dose of vaccine around April 10, 2021.
It should be noted that May 3, when the delta variant first emerged was about one week after the end of the ‘protective’ or negative excess all cause mortality. This suggests that what ever was contributing to protection from excess all cause mortality may have been protecting against the emergence of the delta variant with a lag time of about 7 days for it to be counteracted.
This reminds me of the fact that Tartof SY et al., (Lancet October 4, 2021 see Appendix 5c) reported that in people over the age of 64, for the first 6 days after administration of the second dose, there was sterilizing immunity (no cases per 100,000/py) but when examined at any time over 6 days, the vaccine effectiveness (VE) against infection dropped from 84 % with a mixed assortment of variants, to 78/86 % with alpha and subsequently 56/44/48 % with delta. It is notable that sterilizing immunity (100 % VE against infection) started and then held for the time up to 6 days post second dose, while alpha and delta variants emerged. Taken together these results seem to imply trained innate immunity can provide sterilizing immunity especially when facing the alpha or delta variants, but is lost upon boosting of the neutralizing antibodies as may be associated with ADE.
The Delta Variant Dominance in Canada (July 12, 2021).
The date at which 50% of the 80+, 70-79 years of age, and 60-69 had been fully vaccinated was June 5, June 12, and June 19 again implying the second doses were administered May 22, May 29 and June 5, respectively. Over 5.496 million highly susceptible Canadians over the age of 59 (as well as a small percentage of less vulnerable people) received the second dose of the COVID-19 vaccine during the time of circulation of the alpha and delta variants.
On July 19, 2021 50% of the Canadian population was fully vaccinated (Slide 8) meaning the second dose was administered at least 14 days earlier (by July 5). According to Tartof (see above), enhanced infectivity/emergence of the delta variant could be possible by day 7 presumably due to ADE. Day 7 would be July 12, 2021. Thus, it is quite possible the 2 dose vaccination protocol selected for the delta variant emergence and subsequently dominance in Canada.
The Issue of Protection or Negative Excess ACM
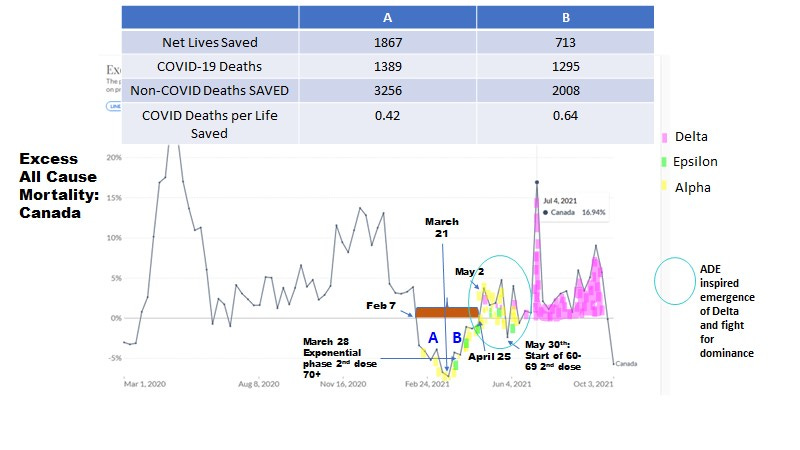
Slide 9. COVID-19 Deaths Per Life Saved
It appears that alpha became dominant by the end of A. It is first detected at 14 % on February 22 (Slide 9 left side of region A) and then 44% by March 22 but it is the most common variant at that time. For the ascent from March 21 to April 25 (region B) we see evidence of alpha and epsilon competing for dominance. On the other hand the delta variant emerged 1 week later after exiting the protector phase B (at 1%). The date of dominance however, coincided with over 50% of the Canadian population receiving the second dose one week earlier on July 12, 2021. This provides substantial evidence linking the inflection points on the EACM profile with selection of variants. But there is more.
The table in Slide 9 gives the data for the negative ACM for A (Feb 10 to March 21, 2021) and that for B (March 21 to April 28, 2021). In the left side of the trough (A) we have less COVID-19 deaths per life saved (0.42) when compared with the right side at B, where there were more (0.64), meaning the heterologous protection by trained innate immunity is stronger in A than in B against COVID-19. The protection mechanism against COVID-19 which also protects against non-COVID disease (eg, cancer, cardiovascular, diabetes etc.) became weaker in region B than region A (compare 3256 non-COVID lives saved in A to 2008 in B). Put another way, 2 dose vaccination via ADE counteracts sterilizing immunity by trained innate immunity and is detrimental if the person is infected with SARS-CoV-2, but otherwise if there is no SARS-CoV-2 infection, it is less likely to interfere with protection. Note that on the B side there are many or a mix of variants trying to dominate when presumably the antibodies to spike protein receptor binding domain and neutralizing antibodies are interfering with sterilizing immunity by the innate system.
Thus, there may be a correlation of vaccine-induced ADE interference inhibiting trained innate immunity and the heterologous protection against SARS-CoV-2 variants.
It is noteworthy that the heterologous protection against mortality from January 3, 2021 to April 28, 2021 which peaked around March 21, 2021 involved both COVID-19 and non-COVID deaths (Slide 6). It is believed that trained innate immunity provides sterilizing immunity against infection with variants (Tartof SY et al., (Lancet October 4, 2021 see Appendix 5c). However especially in the frail mere vaccination with one dose of vaccine may induce death with revised estimates in the USA at 24 per million (*Lv G et al., Front Med, 14 May 2021).
[*Note that they said there were 55 deaths per 6,688,231 vaccinated from December 11, 2020 to January 8, 2021. However from the Our World in Data there was 0.69 % of the USA population vaccinated by January 8, 2021 (0.68 % with one dose only) which for a population of 332.9 million was 2.297 million vaccinated. Thus, this increased the rate from 8.2 per million to 24 per million.]
This may have helped flatten the COVID-19 mortality and ICU admissions from January 3 to April 28, 2021 for Canada when compared with the UK and the USA (see slide 10). On the other hand, Canada had fewer cases, ICU admissions and deaths per 1 million than the UK and the USA (Slide 10) overall.
[NB: No data available at Our World in Data for Canada for hospitalizations.].
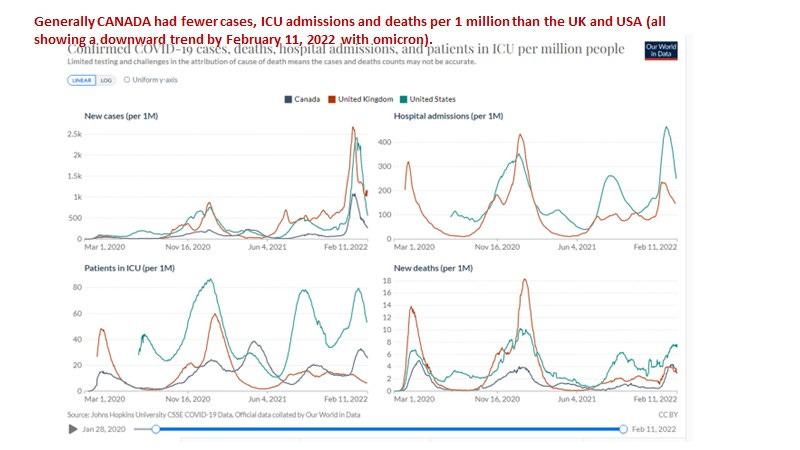
Slide 10. Canada was hit the least by the pandemic per capita when compared with the UK and the USA.
Potential Contribution of NACI Policy on Reducing Deaths During the Pandemic
There may be many reasons for why Canada suffered less than the USA (less obesity, better health care, better education, federal government support during the lockdowns) but I think the National Advisory Committee on Immunization (NACI) deserves some credit for a health protection policy which may have favored innate immunity over adaptive and may have either saved more lives or blocked a more rapid emergence or dominance of variants.
As announced on April 7, 2021 but likely implemented by February 27, 2021 (Slide 8), NACI extended the interval between the first and second doses of COVID-19 vaccine due to limited vaccine supply. This approach was meant to provide more people with 80% protection by ‘temporary’ innate immunity rather than far fewer people with 90% protection against infection (adaptive immunity with neutralizing and spike RBD binding antibodies).
Aside from January 17, 2021 (Slide 8) and the period February 14 to 28, 2021 (Slide 8), the NACI policy recommendation, did lead to a significant decrease in the two/one dose ratio which remained at 0.227 or lower from March 22, 2021 to about June 14, 2021 (Slide 8). At this inflection point about 52 % of Canadians had received the first dose while only 13.1 % had received the second dose. While most countries suffering the pandemic did show a negative EACM period, it should be noted that two countries did not exhibit any significant negative EACM; Israel and Italy. For these two countries the ratio (two dose/one dose) generally exceeded the >0.5 cutoff (Slide 8) throughout the vaccination period.
Due to the substantial benefit of heterologous protection against non-COVID-19 deaths and COVID-19 deaths from January 3 to March 21 2021 (Slide 6), it is difficult to say whether the second dose should have been administered at all, merely delayed longer to say 6 months, or instead an innate immunity vaccine such as the BCG vaccine should have been administered instead of the second COVID-19 vaccine dose. It may be difficult to move forward on resolving this dilemma as it would be difficult to conduct randomized clinical trials to test these various protocols if the pandemic has or is ending.
Summary
Taken altogether in Canada there was clear evidence for selection of variants of concern by two doses of the COVID-19 vaccine.
The selection for the alpha variant emergence in Canada occurred around February 22 and dominance occurred by March 22, 2021 (region B in Slide 9). The delta variant emerged about 1 week (May 3) after the exit from the “protector phase” (region A and B in Slide 9) and battled with alpha (blue circle in Slide 9 and epsilon) before establishing dominance around July 12, 2021 (at 52 %) and at 98% by about August 15, 2021. The date of delta dominance coincided with over 50% of the Canadian population receiving the second dose one week earlier.
The emergence and then dominance of the alpha and delta variants occurred either when the two dose to one dose ratio exceeded 0.50 (alpha emergence and delta dominance) or when the heterologous protection of one dose significantly dropped (alpha dominance and delta emergence) as demonstrated by significant inflection points in the excess all cause mortality plot.
The EACM analysis gives us clear evidence that the protection during the ‘negative’ excess all cause mortality period was associated with heterologous protection against the common non-COVID causes of death in addition to COVID-19 mortality. This protection weakened as relatively more second doses were administered and was associated with higher COVID-19 deaths per life saved. Coincident with this weakening we see indirect evidence of ADE by the emergence and then dominance of alpha, then delta. As anticipated, here it is documented at a population level that innate immunity heterologous protection against COVID-19 is lost with selection of more transmissible variants (presumed ADE) associated with administration of the second COVID-19 vaccine dose.
Fishman DN & Tuite AR (medRxiv August 4, 2021) have shown for Ontario residents that the alpha variant was more virulent than the the wild type, while the delta variant was more virulent than alpha. Both variants significantly showed increased risks for hospitalization, ICU admission and death over the wild type. Thus, it follows that selection by two dose vaccination was not only for more transmissible variants but for more pathogenic strains in Canada.
To summarize it is not clear that two dose adaptive immunity vaccines were appropriate for use during pandemics with emerging RNA viruses (Slides 2, 6, 8 & 9) due to the selection of more transmissible and pathogenic variants. This only served to prolong the pandemic as well as the lockdowns. In response to the failure of the two dose adaptive immunity approach to contain the pandemic, public health officials invoked boosting protocols and vaccine mandates which caused further economic hardship and calamity. However, boosting with the same Wuhan wild type strain spike protein would only serve to select for more highly transmissible variants in the population rendering herd immunity more evasive. Indeed, the UKHSA has documented (see vaccine surveillance weekly documents available on their website) first with delta and now with the onset of the omicron variant that the two dose (or more) vaccinated are at higher risk of symptomatic infection than the unvaccinated per 100,000 as stratified by age. This means despite rhetoric to the contrary, since the arrival of the delta variant it has been the vaccinated who are driving infections and perpetuating the pandemic. Furthermore, the safety of these EUA vaccines have not been properly assessed and their efficacy against hospitalization and death were not studied at the randomized clinical trial level. All of the above would surely invalidate the mandating of an experimental vaccine not to mention these mandates are patently unconstitutional.
Although an omicron specific spike mRNA vaccine is under clinical trial assessment, its use is predicted to be potentially catastrophic or at best redundant, as many if not most people have already been naturally immunized to omicron.
Conclusions
Given the uncertainty of : i) what approach for vaccination would have been best (adaptive versus innate, Slide 1), ii) the anticipated (Slide 1) and here validated risk of selection for more infectious and pathogenic emerging RNA virus variants by adaptive immunity vaccines with prolongation of the pandemic, and iii) the overall lack of safety assessment for the adaptive immunity COVID-19 vaccines, alternatives to vaccination should have been considered and implemented.
Immunosenescence (Laderoute M, Discovery Medicine, 2015, 2020), not only is a critical risk factor determining COVID-19 severity but also for vaccine failure and untoward vaccine side effects all of which increase with age. This means most of the population, especially the elders and most vulnerable, may have been better served simply by strategies to prevent and reverse immunosenescence. It is noteworthy that I advocated this approach on LinkedIn on March 5, 2020 before the pandemic was declared on March 11, 2020 in my article entitled ‘The HERV-K Way to Keep Coronaviruses at Bay’. {This paper is now available at hervk102@substack.com.} In addition to zinc and flavonoids which reverse immunosenescence by inactivating alpha-fetoprotein (Laderoute M, 2015, 2020), elsewhere it is argued that ivermectin may also be an alpha-fetoprotein antagonist which may specifically reverse SARS-CoV-2 induced immunosenescence (Laderoute MP, Open Heart, April 29, 2021. [https://openheart.bmj.com/content/8/1/e001655.responses#ivermectin-may-prevent-and-reverse-immunosenescence-by-antagonizing-alpha-fetoprotein-and-downmodulating-pi3k-akt-mtor-hyperactivity] ). Newer evidence suggests Vitamin D and/or ivermectin may ameliorate the transition of LB- foamy M1-like macrophages (which produce trained innate immunity through the production and lytic release of HERV-K102 particles) to LB+ foamy M2 macrophages which are not protective (see new article called “Ivermectin’s Little Secret” Feb 28, 2022 at hervk102@substack.com).
In conclusion, despite the short-term benefit of heterologous protection against excess all cause mortality associated with the administration of one dose, the lockdowns could have been best avoided, and numerous lives saved if only we implemented the test and treat strategy with cheap and effective off label drugs such as ivermectin, the latter which has been shown to be effective against COVID-19 severity (Kory P et al., Am J Therapy April 2021 and see also https://c19early.com/).
I have read and appreciated your 4 articles- I had to go back to 2007 to review the chemistry.
For further analysis it would be interesting to overlay the 2020 and 2021 data. 2020 behaved as expected for a seasonal respiratory virus- mostly done by the spring and the summer was fairly benign. This contrasted with 2021 which demonstrated the unseasonal peaks which you have explained. I had assumed that there was a direct toxic effect of the injections as well- the VAERS post-injection mortality has been widely discussed on Substack.
The Canadian data would be challenging to compare with anywhere else in the world due to the "Mix-and Match" supplies of the various injections, and the somewhat randomly extended inter-administration intervals.
My former colleagues and administration were all enthusiastic about the minimal protective effects you have elucidated, and willfully dismissive of the risks, to the point that they were all eager to have their children injected. Of course prophylaxis and early treatment as you have suggested were mocked and dismissed.