

We are at a Cross-Road with the Pandemic
We are at a Cross-Road with the Pandemic
July 30 2022

I think it is fair to say that Bill Gates got it right in his comments about widespread omicron infection that the risks of severe COVID-19 disease are dramatically reduced by this exposure, although I would replace the word “sadly” with “amazingly”.
He went on to say that SARS-CoV-2 would become endemic just like influenza with little chance of significant development of variants, and thus, the pandemic would end.
I should say that would have been correct if only we stopped using the COVID-19 vaccines after the second dose. Indeed if we did not use the vaccines at all, and stuck with early prevention and intervention treatments proven to work, the pandemic would have been quenched … stopped in its tracks, at least by early 2021 [1,2]. It is this non-divine intervention called SARS-CoV-2 vaccination (adaptive immunity; spike specific) that is postponing the end of the pandemic [3].
It is notable that the selection of SARS-CoV-2 immune escape variants was EXCLUSIVELY a result of the SARS-CoV-2 vaccines although a role of neutralizing monoclonal antibodies used for therapy cannot be discounted [3]. If you examine the emergence of the alpha and delta variants globally at Our World in Data [https://ourworldindata.org/coronavirus], it is blatantly clear that for the first year of the pandemic before widespread vaccination occurred, there wasn’t much in terms of the selection of immune escape variants. The exceptions were of course those countries which participated in vaccine randomized controlled trials, such as the 637,379 participants in the UK [https://www.gov.uk/government/news/over-half-a-million-people-taking-part-in-pioneering-covid-19-research] which saw the early emergence of the alpha variant in November/December 2020. The conundrum of trying to end a pandemic by implementing, let alone mandating strategies that prolong it, is something the the public health authorities will need to explain.
The carnage that the COVID-19 vaccines especially the mRNA (gene therapy) vaccines, have placed on populations near and far [4,5] is astounding. More worrisome is that nothing is being done by the regulatory authorities to rein this in. As of Friday, July 29, 2022, the VAERS database including foreign reports contains 19,236 deaths linked to the Pfizer-BioNTech mRNA COVID-19 vaccine; 7,917 with the Moderna mRNA COVID-19 vaccine, and 2,584 with the Johnson and Johnson COVID-19 vaccine, and which most certainly represent just the tip of the iceberg. This contrasts with the mere 25 deaths that resulted in the removal of the Swine Influenza Vaccine from the market in 1976 by the US FDA [6]. Is the FDA sleeping, drugged or of a different allegiance?
HESN: Lessons From HIV-1; A Concurrent RNA Pandemic Virus
Few people understand the critical importance of innate immunity of humans in its defense against emerging or pandemic RNA viruses. The havoc that virus-specific antibodies can have on outcomes such as antibody dependent enhancement (ADE) of infection into macrophages is nothing short of deadly.
In HIV-1, the existence of subsets of the population who are regularly exposed to HIV-1 yet show protracted resistance against acquisition are called “HIV-1 Exposed SeroNegative (HESN)” cohorts. As the name suggests, supreme protection against HIV-1 acquisition correlates with a notable absence of antibodies to HIV-1 specific viral antigens in these very special individuals. In the world of RNA pandemic responses, no virus specific antibody is a good thing.
Similarly in COVID-19, antibodies to spike protein are associated with COVID-19 disease progression and not protection [reviewed in 3]. There was an early report that an unknown innate response related to decreased hs-CRP levels may promote recovery in mild COVID-19 patients associated with younger age (15 to 39 years of age) [7]. In contrast, high levels of spike neutralizing antibodies (NAbs) were associated with elevated CRP as was found in the older age group (60-85 years of age) and this was associated with longer hospital stays. About 36.7 % of the recovered mild patients (n=175) had very low levels or negligible levels of NAbs whereas 10/175 completely lacked NAbs reminiscent of the HESN. The latter group had the shortest hospital stays and were dominated by women under the age of 40 in 8 of the 10 cases. Clearly SARS-CoV-2 Exposed SeroNegative (SERN) individuals exist and like the HESN, it would be fruitful to understand the mechanisms involved. Interestingly vitamin D deficiency hastens HIV-1 progression to AIDS [8] and cholesterol metabolism and perhaps trained (innate) immunity figure prominently in the HESN phenotype [9].
A candidate correlate of protection against COVID-19 severity was recently identified as the HERV-K102 trained innate immunity that occurs in lipid body negative foamy macrophages (LB-FMs) [3] as shown in Image 1 (bottom panel). In the bronchoalveolar lavage fluids (BALF) these LB-FMs correlate with recovery from moderate COVID-19 and are depleted with progression to severity associated with ADE [reviewed in 3].
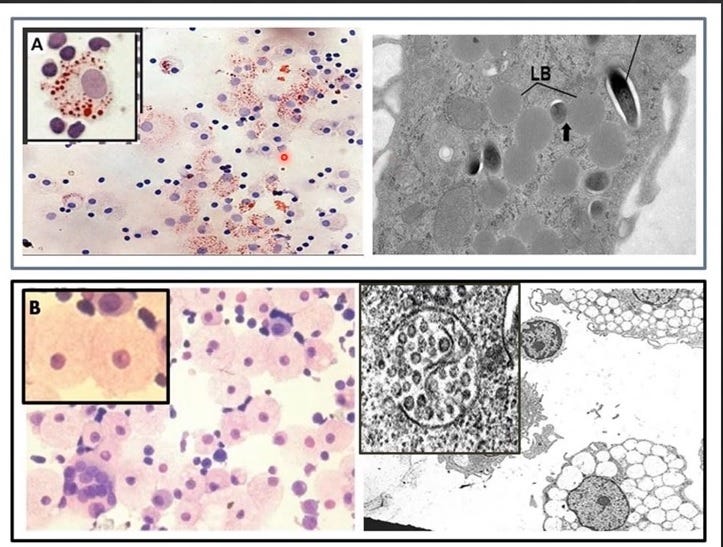
Image 1. Two Types of Foamy Macrophages
A) The lipid body positive foamy macrophages (LB+FMs) are Oil Red O strongly positive due to the storing of cholesterol as esterified cholesterol (CE) in the lipid bodies (LB) and which are considered M2-like and anti-infammatory). Top panel from [10].
B) The lipid body negative foamy macrophages (LB-FMs) which do not stain well with Oil Red O are highly vacuolated and produce copious amounts of protector HERV-K102 particles. They are M1-like, pro-inflammatory and amplify interferon responses [reviewed in 3]. Bottom panel from [11].
Note that many intracellular pathogens including SARS-CoV-2 and other viruses upon infection of macrophages convert the LB-FMs to LB+FMs as a form of immune escape and to favor their replication [12].
In BALF, only the LB-FMs and their progenitors (the CD14+CD16+ monocytes) express highly active VDR, the receptor for vitamin D (out of 66 different cell types). Vitamin D deficiency promotes the conversion of LB-FMs to LB+FMs, abrogating the HERV-K102 trained immunity defense mechanism [reviewed in 3] and providing immune escape for SARS-CoV-2 allowing its replication [12].
Getting back to the SESN, one has to wonder why for both HESN and SESN cohorts, women under the age of 40 tend to be over-represented. Given that HERV-K HML-2 [13] or HERV-K102 [14] full length RNA transcripts are induced by estrogen followed by progesterone in vitro and this occurs at the time of ovulation in women in vivo [15], this raises the possibility that women of child-bearing age may be more likely to have preactivated HERV-K102 trained immunity protection. This might allow for more rapid SARS-CoV-2 clearance and recovery while potentially, precluding the development of the deadly SARS-CoV-2 specific antibodies during natural infection. This hypothesis is easily testable and is worthy of further investigation. It is also likely that children are protected by common exposures to viruses which would induce HERV-K102 particle production [16] frequently reaching levels at 10 (11) particles per ml of plasma. Again, this needs to be directly examined.
Is it true as Bill Gates has suggested that omicron generates both B cell and T cell adaptive immunity to SARS-CoV-2 specific antigens which will end the pandemic?
A recent report on triple-vaccinated health care workers in the UK and subsequent effects of omicron infection on adaptive immunity revealed considerable subversion (inhibition) of SARS-CoV-2 antigen recognition at both the B cell and T cell levels following omicron infection [17]. Immune imprinting by a natural SARS-CoV-2 infection earlier in the pandemic was associated with the abrogation of neutralizing antibodies (NAbs) and T cells to omicron but not to earlier variants. Those without a previous natural infection showed some T cell responses and NAbs to omicron, but much stronger responses to earlier variants. The authors suggested imprinting impaired omicron boosted SARS-CoV-2 responses and insinuated (but did not state) that this might compromise protection. This imprinted tolerance induction has raised eyebrows about whether omicron is the panacea of divine intervention or a harbinger of a disaster yet-to-come.
Why Omicron is the Panacea to End the Pandemic, Provided We STOP COVID-19 Vaccines Immediately
As argued above, SESN is the preferred option to generate herd immunity (see Image 2), and to prevent ADE mediated selection of immune escape variants which prolongs the pandemic. In Image 2, the evidence shows boosted trained immunity can generate sterilizing immunity against the alpha and delta variants.
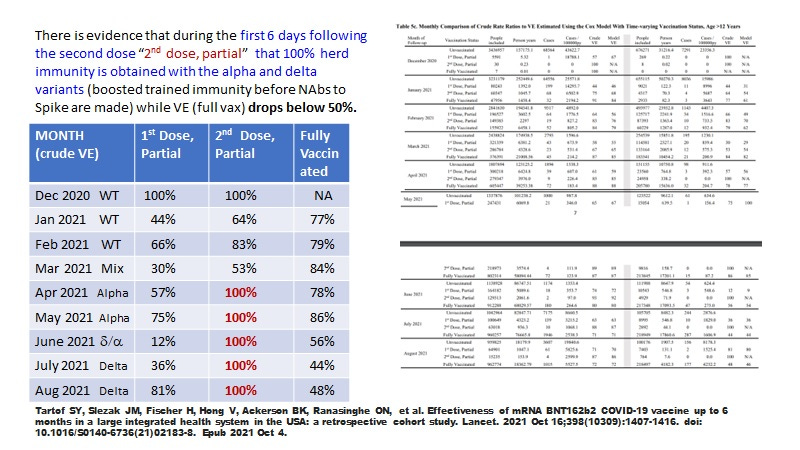
Image 2. Evidence That Boosted Trained Innate Immunity (Demonstrated During the First 6 Days After the Second mRNA Vaccine Administration But Not After) is Capable of 100% Vaccine Effectiveness (VE) Against Symptomatic Infection for the Alpha and Delta Variants, While the VE for the Fully Vaccinated Drops Below 50 % for Delta [18].
Data consistent with the notion that trained innate immunity can provide about 97 % or better protection against Omicron associated mortality is shown in Images 3 to 6. Omicron variants around June 6 2022 were a mix of BA.2, BA.5, BA.4 and BA2.12.1. Image 3 plots the Excess All-Cause Mortality (EACM) over COVID-19 deaths per million and shows: 1) associated with vaccination there are periods where substantial negative EACM can be detected; 2) shortly after the onset of omicron deaths, negative EACM was detected despite significant SARS-COV-2 associated deaths, some of which probably related to vaccine toxicity from immunization of the third vaccine dose around December 22, 2021 (Image 4) and/or the fourth vaccine doses around late April 2022. In Image 5, in the UK a week of significant absence of deaths is noted for the week ending on June 3, 2022, which corresponds to June 5, in Image 6. A rough estimate is that about 390 individuals died in any given week in the UK during the omicron wave, but for the week ending June 3, 2022 it may have been 10 providing roughly a RR against death of 0.03 or about 97% protection against death. Trained innate immunity involves HERV-K102 particle production [3] and is known to provide heterologous protection against death [reviewed in 3]. The non-COVID-19 deaths captured in Image 3 could include deaths induced by the toxicity of the mRNA vaccines but this needs to be investigated and verified.

Image 3. Plot of Excess All-Cause Mortality (EACM) Layered Over COVID-19 Deaths per Million Illustrating Negative EACM and Non-COVID-19 EACM
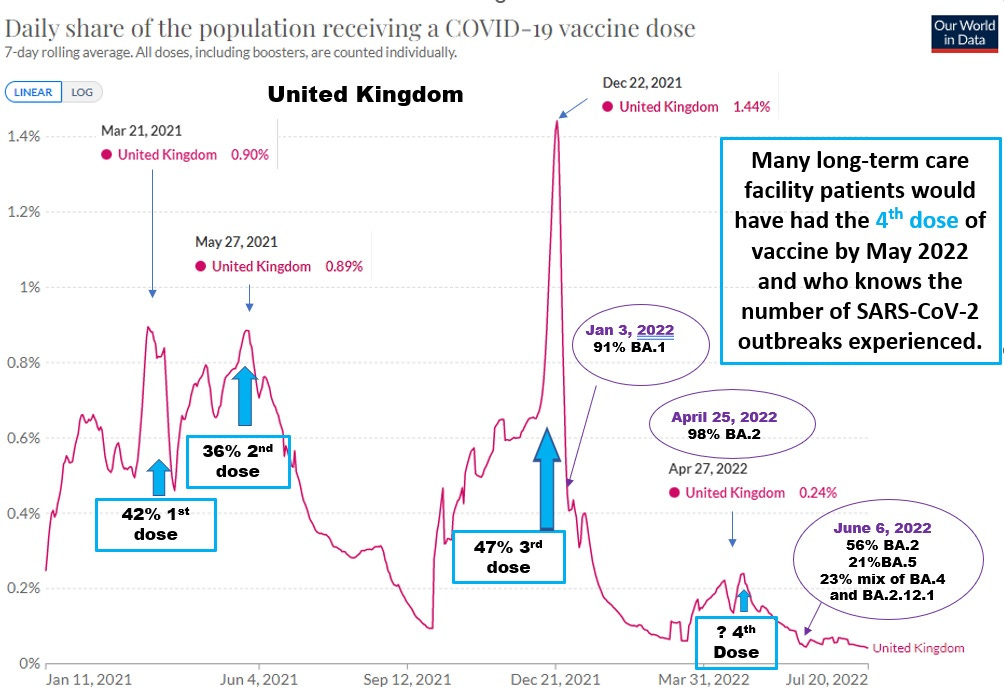
Image 4. Share of UK population receiving a COVID-19 Vaccine Dose.
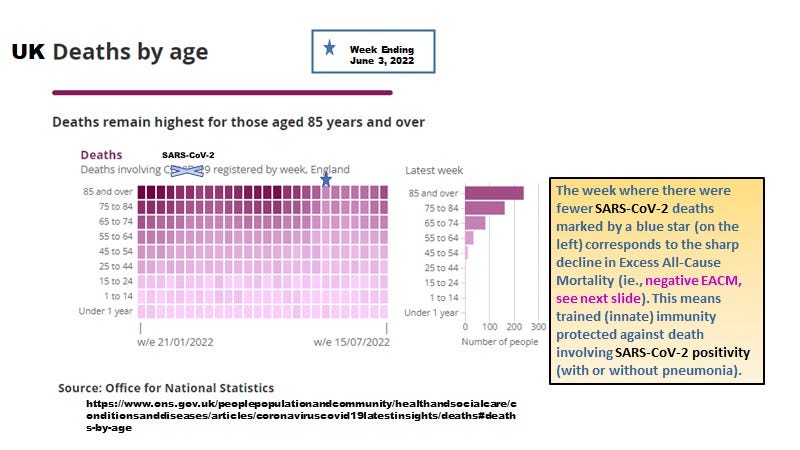
Image 5. UK Weekly Deaths By Age in the Omicron Era
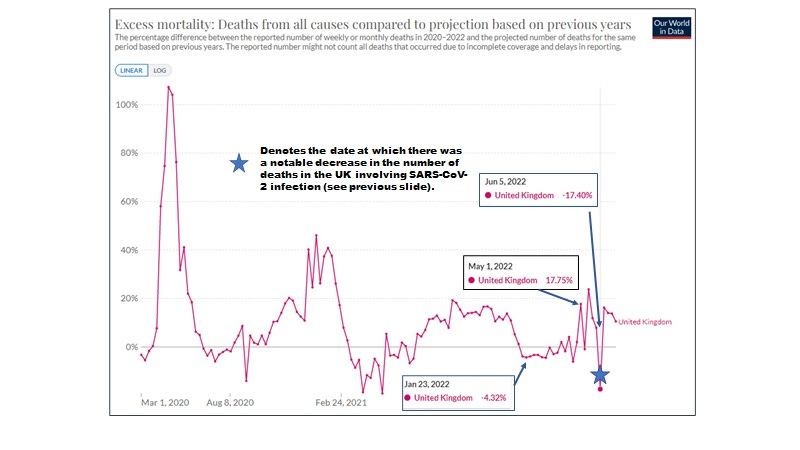
Image 6. June 5,2022 Showed a Negative EACM of -17% Around the Time of Almost No Deaths Involving SARS-CoV-2 for Week ending June 3, 2022 in Image 5.
In summary we see that omicron and variants may induce negative EACM suggestive of trained innate immunity needed to end the pandemic. However, the repeated exposures to the vaccines may interfere with maintaining trained innate immunity and due to the toxicity of the vaccines especially the mRNA spike vaccines, may be contributing to deaths with and without SARS-CoV-2 exposures. In order to end the pandemic, all vaccination must cease. Instead, prevention and early treatment protocols [1,2] should be prioritized for our elders and especially at long term care facilities.
Whether we sink or swim out of this pandemic relies heavily on the willingness of regulatory bodies like the FDA to rescind EUA and market approval for the deadly and pro-pandemic COVID-19 vaccines.
References
McCullough PA, Alexander PE, Armstrong R, Arvinte C, Bain AF, Bartlett RP, et al. Multifaceted highly targeted sequential multidrug treatment of early ambulatory high-risk SARS-CoV-2 infection (COVID-19). Rev Cardiovasc Med. 2020 Dec 30;21(4):517-530. doi: 10.31083/j.rcm.2020.04.264.
Kory P, Meduri GU, Iglesias J, Varon J, Cadegiani FA, Marik PE. "MATH+" multi-modal hospital treatment protocol for COVID-19 infection: clinical and scientific rationale. J Clin Med Res. 2022 Feb;14(2):53-79. doi: 10.14740/jocmr4658.
Laderoute MP. Trained immunity involving HERV-K102 activation may promote recovery from COVID-19 providing a new vaccination paradigm against pandemic RNA viruses. (Submitted: July 26, 2022).
Seneff S, Nigh G, Kyriakopoulos AM, McCullough PA. Innate immune suppression by SARS-CoV-2 mRNA vaccinations: The role of G-quadruplexes, exosomes, and microRNAs. Food Chem Toxicol. 2022 Jun;164:113008. doi: 10.1016/j.fct.2022.113008.
Laderoute M. Spike Toxicity in the UK Elder and Males from Alberta, Canada. July 29, 2022. https://hervk102.substack.com.
McCullough PA. Safety Concerns Regarding the COVID-19 Vaccine. October 15, 2021, www.americaoutloud.com.
Wu F, Liu M, Wang A, Lu L, Wang Q, Gu C, et al. Evaluating the association of clinical characteristics with neutralizing antibody levels in patients who have recovered from mild COVID-19 in Shanghai, China. JAMA Intern Med. 2020 Oct 1;180(10):1356-1362. doi: 10.1001/jamainternmed.2020.4616.
Fenizia C, Saulle I, Clerici M, Biasin M. Genetic and epigenetic regulation of natural resistance to HIV-1 infection: new approaches to unveil the HESN secret. Expert Rev Clin Immunol. 2020 Apr;16(4):429-445. doi: 10.1080/1744666X.2020.1732820.
Saulle I, Ibba SV, Vittori C, Fenizia C, Mercurio V, Vichi F, Caputo SL, Trabattoni D, Clerici M, Biasin M. Sterol metabolism modulates susceptibility to HIV-1 Infection. AIDS. 2020 Sep 1;34(11):1593-1602. doi: 10.1097/QAD.0000000000002591.
Peyron P, et al. Foamy macrophages from tuberculous patients' granulomas constitute a nutrient-rich reservoir for M. tuberculosis persistence. PLoS Pathog. 2008 Nov;4(11):e1000204. doi: 10.1371/journal.ppat.1000204.
Laderoute MP. Clues to finding correlates of risk/protection for HIV-1 vaccines [version 2; peer review: 2 approved with reservations] F1000 Research 2018, 6:868. https://doi.org/10.12688/f1000research.11818.2.
Dias SSG, Soares VC, Ferreira AC, Sacramento CQ, Fintelman-Rodrigues N, Temerozo JR, et al. Lipid droplets fuel SARS-CoV-2 replication and production of inflammatory mediators. PLoS Pathog. 2020 Dec 16;16(12):e1009127. doi: 10.1371/journal.ppat.1009127.
Ono M, Kawakami M, Ushikubo H. Stimulation of expression of the human endogenous retrovirus genome by female steroid hormones in human breast cancer cell line T47D. J Virol. 1987 Jun;61(6):2059-62. doi: 10.1128/JVI.61.6.2059-2062.1987.
Wang-Johanning F, Frost AR, Jian B, Epp L, Lu DW, Johanning GL. Quantitation of HERV-K env gene expression and splicing in human breast cancer. Oncogene. 2003 Mar 13;22(10):1528-35. doi: 10.1038/sj.onc.1206241.
Holesh JE, Bass AN, Lord M. Physiology, Ovulation. [Updated 2021 May 9]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK441996/
Laderoute MP, Giulivi A, Larocque L, Bellfoy D, Hou Y, Wu HX, et al. The replicative activity of human endogenous retrovirus K102 (HERV-K102) with HIV viremia. AIDS. 2007 Nov 30;21(18):2417-24.
Reynolds CJ, et al. Immune boosting by B.1.1.529 (Omicron) depends on previous SARS-CoV-2 exposure. Science. 2022 Jul 15;377(6603):eabq1841. doi: 10.1126/science.abq1841.
Tartof SY, et al. Effectiveness of a third dose of BNT162b2 mRNA COVID-19 vaccine in a large US health system: A retrospective cohort study. Lancet Reg Health Am. 2022 May;9:100198. doi: 10.1016/j.lana.2022.100198.
Note added after posting. If we look at Image 3, we see that for the most part, between January 11, 2022 to July 3, 2022, the excess all-cause mortality (EACM) was negative. During this time there were 99.49 excess deaths per million over the same period for 2015 to 2019. There were 443.94 COVID-19 deaths per million from January 11, 2022 to July 3, 2022. The difference of 344.45 deaths per million represents the lives saved by "the induction of trained innate immunity" by omicron exposure. This is about 22,734 non-COVID-19 deaths averted by omicron exposure for the UK (population of about 66 million) during this period.
Ab initio I have been looking for two matters that none of my sources had really discussed or touched upon:
1. What are the mechanisms of action of C19? I need to know more than that it is respiratory in nature.
2. What is the minimum infection dosage for c19? I know that if PCR CT >24 the virons are not culturable and hence not infectious. I want to know the min load.
Have you seen any citations for those two matters?