

Trends in Symptoms with Serious Adverse Events of the mRNA COVID-19 Vaccines
Trends in Symptoms with Serious Adverse Events of the mRNA COVID-19 Vaccines
A Call for an International Database of Therapeutic Interventions

Ivermectin as a main therapeutic agent for treatment of Long COVID and/or COVID Vaccine Injury does not always reverse disease.
In either clinical disease, it is the toxicity of the spike protein thought to induce disease.
The presence of spike IgG1/IgG3 (which are dangerous) versus spike IgG4 (the latter associated with the third dose and considered tolerogenic) induced by the vaccine may influence outcome. For example, the dangerous IgG isotypes to spike protein may target and lead to higher infestation rates of the spike protein into macrophages.
Delays of a minimal of 14 to 21 days before onset of diseases following vaccination (especially the second dose) might suggest the spike antibodies could play a role in the disease.
When the disease strikes early such as within 24 hours, it could be due to injection right into the blood such as for pulmonary emboli (the most frequent side effect in women).
The duration of contamination such as for peripheral blood mononuclear cell monocytes which can be up to 15 months also likely plays a major role [1]. In the post-market surveillance of a very immunosuppressive monoclonal antibody (to macrophages) which was removed from the global market in 2009, the incidence of myocardial infarction (MI) although relatively rare during the first 3 months of use, doubled about every 3 months (unpublished observations and where the idea for immunosenescence and causing cardiovascular diseases came from). Accordingly, the longer the duration of immunosenescence the worse or more serious the disease. Also if there is another infection (including SARS-CoV-2) this will further provoke immunosenescence and may cause “rapid progression”.
It has been said that the S2 protein which lingers or is more highly expressed with the COVID-19 mRNA vaccines when compared with natural infection interferes with P53 and BRCA1/2 [2]. This can lead to cancer (in non-myeloid cells) and/or immunosenescence [3,4] if the myeloid cells (the monocytes and macrophages) become infected with SARS-COV-2 (Long COVID) or infested with spike protein (COVID Vaccine Injury).
Immunosenescence of macrophages has been defined as the failed lytic release of protector HERV-K102 particles from foamy macrophages [3,4]. The foamy macrophages producing the protector HERV-K102 foamy virus particles are shown in Figure 1 [5,6].
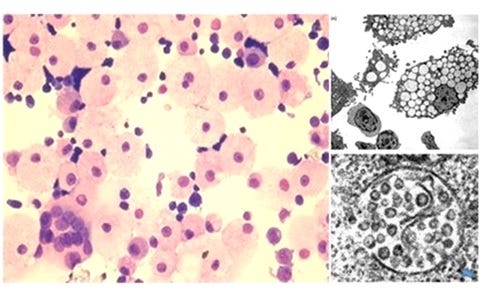
Figure 1. HERV-K102 Particle Production in Cord Blood Mononuclear Cells (CB) Cultured in IMDM Media [5,6]
Left image: H&E staining of CB cytospins showing the dominant presence of highly vacuolated foamy macrophages amongst normal small lymphocytes (400X) when CB is cultured in IMDM. Note the presence of a rare multinucleated giant macrophage. Right image top: Electron microscopy of vacuolating CB cells day 11 at 1500X. Right image bottom: At 100,000X immature particles (the centers are not condensed) can be seen in the vacuoles which averaged about 100 nm. Envelope spikes are also noted. No cell surface budding was observed by EM. Release of the particles occurred on day 6-7 by lysis. Note that when CB was cultured in RPMI this aborted foam cell formation. Also, the addition of IL-2 and PHA aborted foam cell formation in IMDM cultures implying adaptive immunity may downmodulate HERV-K102 particle production. Blue arrows point to the preassembly of envelope with gag as aggregates in the trans-golgi network which then bud into the vacuoles. This assembly which requires envelope protein is characteristic of foamy retroviruses but not orthoretroviruses.
In Figure 2 it is shown that alpha-fetoprotein (AFP) causes immunosenescence of macrophages and that AFP antagonists (isoflavonoids) reverse immunosenescence. These known antagonists include zinc, flavonoids, DHEA or 7-keto-DHEA, and more recently ivermectin [7].
One should note that AFP confers the malignant phenotype (oncoprotein) and is known to be associated with cancer initiation and progression [7]. Thus, it follows since ivermectin may bind and inactivate AFP, that ivermectin has anti-cancer, anti-viral properties and can reverse immunosenescence the cause of chronic illness and which blocks immune surveillance against infectious agents and cancers.

Figure 2. The New Immunosenescence Paradigm, 2015 [3,4]
In the new immunosenescence paradigm, active alpha-fetoprotein (AFP) was proposed to mediate immunosenescence of macrophages, defined as the failed lytic release of HERV-K102 particles from foamy macrophages [3,4]. AFP blocks apoptosis in macrophages. The activity of AFP depends in part on the DHEA/cortisol ratio which diminishes with age and/or stress. This is because cortisol induces AFP while DHEA binds and renders AFP inactive [3]. Thus, with age and/or stress there will be more active AFP in the system and a higher risk of immunosenescence. Flavonoids and zinc may reverse immunosenescence by binding and inhibiting AFP activity and thus, will appear to have antiviral properties. Recent evidence is also consistent with ivermectin reversing immunosenescence [7].
In Figure 3, it is shown that there are two types of foamy macrophages in humans. The good ones (B) produce the protector HERV-K102 particles and confer ‘trained INNATE immunity’. The bad ones (A) allow for unbridled production and release of pathogens including SARS-COV-2 [9]. The same occurs in the monocytes in peripheral blood samples [9].

Figure 3. Two TYPES of Foamy Macrophages in HUMANS
A) The lipid body (LB) positive foamy macrophages (LB+FMs) are strongly stained by Oil Red O, are larger and represent the M2-like anti-inflammatory cells [8]. These cells allow for the production of high levels of infectious agents [9] such as Mycobacterium tuberculosis [8]. Note that TB exposures in vitro induce both the B and A types in culture where with time they all become the A type [8].
B) The lipid body negative foamy macrophages (LB-FMs) producing the HERV-K102 particles (see Figure 1 above).
With time pathogens like Mycobacterium tuberculosis and SARS-COV-2 convert the protector FMs to become factories for the production and release of pathogens [9].
In Figure 4, we see how the IgG1 and IgG3 antibodies to spike protein mediate antibody dependent (ADE) enhancement of SARS-CoV-2 infection into macrophages which causes IMMUNOSENESCENCE. It is thought with the production of these dangerous antibodies following the second dose, that this would also enhance spike protein infestation in these macrophages preferentially… also causing IMMUNOSENESCENCE.
IMMUNOSENESCENCE causes chronic diseases like cancer, cardiovascular diseases, autoimmunity, neurological degeneration etc [3,4] in addition to increasing the risks of infections and the risk for reactivation of dormant viruses.
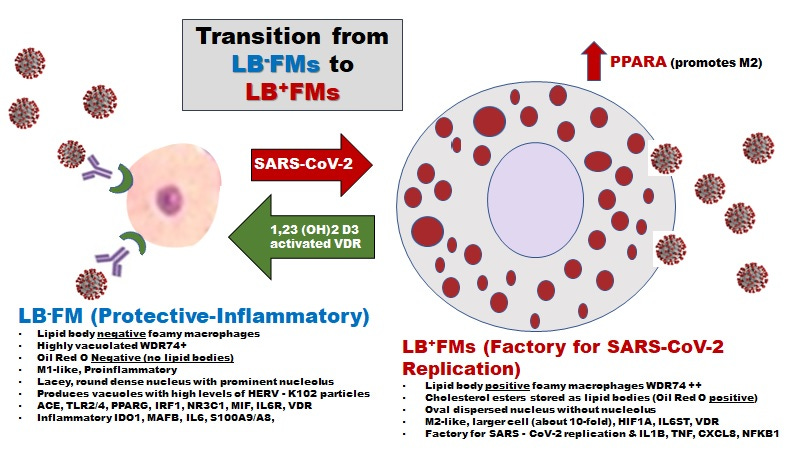
Figure 4. SARS-CoV-2 Infection of the LB-FMs by ADE Causes the Transition to LB+FMs but is Blocked by the Activated VDR [10]
SARS-CoV-2 converts the M1-like protector foamy macrophages (LB-FMs) to M2-like LB+FMs, the latter which becomes a factory for SARS-CoV-2 replication [9]. When the levels of vitamin D3 are sufficient, the activated vitamin D receptor (VDR) can prevent the phosphorylation of MAPK8 blocking the transition from LB-FMs to LB+FMs [10]. Note it is possible that ivermectin may do the same as MAPK8 is on the ivermectin-protein string interaction network [7]. SARS-CoV-2 infection of the LB-FMs by ADE blocks programmed cell death abrogating the release of the HERV-K102 particles and at the same time inducing immunosenescence of the macrophages which exacerbates chronic illness.
The conversion to LB+FMs also does the same; but now SARS-CoV-2 particles are produced and released by cell surface budding and where NFKB1 acts as the transcription factor for the release of IL-1B, TNF-alpha, and CXCL8 [11]. This creates an immunologically priviledged site possibly secondary to the fact that foamy macrophages may not express the spliced HERV-K102 envelope on their cell surface (unpublished flow cytometry data on the LB-FMs).
In a quest to determine if ivermectin may or may not help certain individuals, there may be patterns in symptoms with certain vaccine adverse effects such as associated with lot numbers and/or manufacturers of COVID-19 vaccines that might be informative. Also certain strains of virus may also cause certain symptoms.
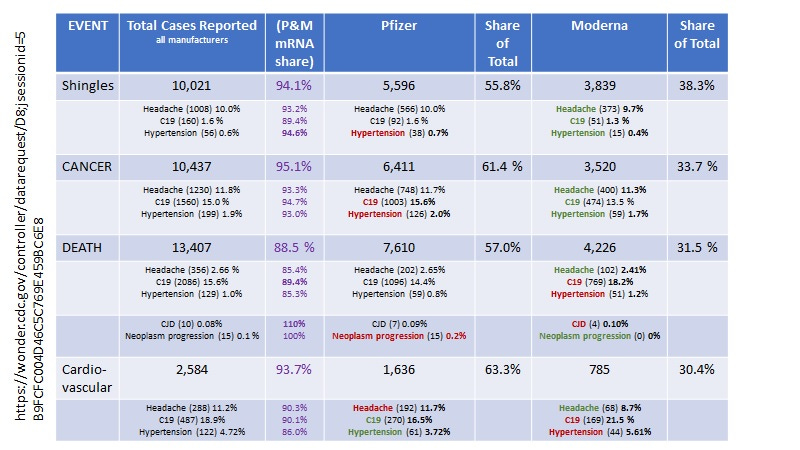
In order to help expedite drug discovery, one might examine the proportionality of symptoms that associate with serious adverse events reported to VAERS by vaccine manufacturer, type and/or lot such as (see Table 1) :
spike protein spread to central nervous system (shingles, headaches);
increased COVID-19 infection positively associated the main events (cardiovascular, cancer, death) but not with others (shingles); and
immunosenescence (hypertension is a sign of immunosenescence) where risk of hypertension in descending order in Table 1 is cardiovascular disease (CVD)>cancer>death>shingles).
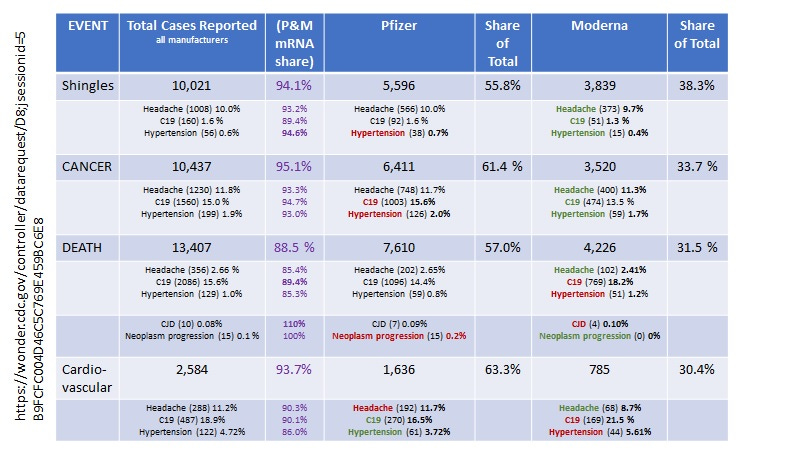
Table 1. Proportionality of Serious Adverse Events by Symptoms and Associations with COVID-19 Vaccine Types at VAERS (September 22, 2023 search at wonder.cdc.gov)
https://wonder.cdc.gov/controller/datarequest/
For example, in Table 1, we see that COVID-19 infection in vaccinated individuals is associated with cardiovascular disease (CVD)> death> and cancer events but not with shingles (reactivation of virus).
By proportions; CVD might be relatively more common in PFIZER vaccinees whereas shingles might be more common in those injected with Moderna vaccines.
The mRNA vaccines might proportionately cause more cancer than the other types of vaccines. However, neoplasm progression was solely a feature of the Pfizer and not the Moderna vaccine. This may provide a hint that there may be other contaminants in the Pfizer vaccine (or at higher levels) which may provoke oncogenesis.
*
Thus, it may be possible by studying these types of associations, to predict what symptoms/individuals might best respond to ivermectin (or other therapeutics) if outcomes from the use of ivermectin and other interventions are carefully recorded along with symptoms of the individuals such as in a common international database using ICD-10 codes.
This knowledge may help clinicians prepare for and address the issue of the best ways to tackle the existing and upcoming litany of “TURBO CANCERS”, considered the next pandemic that we have to face [12].
This is a call to develop an international database of COVID-19/COVID-19 vaccine details with symptoms, lot numbers/variants, manufacturers, and with therapies that worked or not against certain symptoms and serious diseases.
Hopefully, in this way, finding solutions to turbo cancers will be expedited.
REFERENCES
Patterson BK, Francisco EB, Yogendra R, Long E, Pise A, Rodrigues H, Hall E, Herrera M, Parikh P, Guevara-Coto J, Triche TJ, Scott P, Hekmati S, Maglinte D, Chang X, Mora-Rodríguez RA, Mora J. Persistence of SARS CoV-2 S1 Protein in CD16+ Monocytes in Post-Acute Sequelae of COVID-19 (PASC) up to 15 Months Post-Infection. Front Immunol. 2022 Jan 10;12:746021. doi: 10.3389/fimmu.2021.746021.
Singh N, Singh BA. S2 subunit of SARS-CoV-2 interacts with tumor suppressor protein p53 and BRCA: an in silico study. Transl Oncol. 2020 Oct;13(10):100814. doi: 10.1016/j.tranon.2020.100814.
Laderoute MP. A new paradigm about HERV-K102 particle production and blocked release to explain cortisol mediated immunosenescence and age-associated risk of chronic disease. Discov Med. 2015 Dec;20(112):379-91.
Laderoute M. The paradigm of immunosenescence in atherosclerosis-cardiovascular disease (ASCVD). Discov Med. 2020 Jan-Feb;29(156):41-51.
Laderoute MP, Giulivi A, Larocque L, et al. The replicative activity of human endogenous retrovirus K102 (HERV-K102) with HIV viremia. AIDS. 2007 Nov 30;21(18):2417-24.
Laderoute MP, Larocque LJ, Giulivi A, Diaz-Mitoma F. Further evidence that human endogenous retrovirus K102 is a replication competent foamy virus that may antagonize HIV-1 replication. Open AIDS J. 2015 Dec 7;9:112-22. doi: 10.2174/1874613601509010112.
Laderoute M. Ivermectin may prevent and reverse immunosenescence by antagonizing alpha-fetoprotein and downmodulating PI3K/Akt/mTOR hyperactivity. Open Heart. April 29, 2021. https://openheart.bmj.com/content/8/1/e001655.responses#ivermectin-may-prevent-and-reverse-immunosenescence-by-antagonizing-alpha-fetoprotein-and-downmodulating-pi3k-akt-mtor-hyperactivity.
Peyron P, Vaubourgeix J, Poquet Y, et al. Foamy macrophages from tuberculous patients' granulomas constitute a nutrient-rich reservoir for M. tuberculosis persistence. PLoS Pathog. 2008 Nov;4(11):e1000204. doi: 10.1371/journal.ppat.1000204.
Dias SSG, Soares VC, Ferreira AC, et al. Lipid droplets fuel SARS-CoV-2 replication and production of inflammatory mediators. PLoS Pathog. 2020 Dec 16;16(12):e1009127. doi: 10.1371/journal.ppat.1009127.
Oh J, Weng S, Felton SK, et al. 1,25(OH)2 vitamin D inhibits foam cell formation and suppresses macrophage cholesterol uptake in patients with type 2 diabetes mellitus. Circulation. 2009 Aug 25;120(8):687-98. doi: 10.1161/CIRCULATIONAHA.109.856070.
Ren X, Wen W, Fan X, et al. COVID-19 immune features revealed by a large-scale single-cell transcriptome atlas. Cell. 2021 Apr 1;184(7):1895-1913.e19. doi: 10.1016/j.cell.2021.01.053.
Goodyear, Nathan MD. Cancer: The Next Pandemic. February 9, 2023. https://covid19criticalcare.com/cancer-and-spike-protein-whats-the-link/
*Note added:
Apparently the Pfizer mRNA contains SV40 promoters not detected in the Moderna mRNA COVID-19 vaccines. The SV40 nuclear localization signal may further increase the odds of genomic integration of DNA meaning higher chances of insertional mutagenesis causing tumor progression?
For what it is worth: https://wentworthreport.com/the-nipah-virus-and-long-covid/
Do you have an opinion on azvudine for long covid Dr Laderoute? Do any of the HIV drugs have any promise for long covid?