
There are two general mechanisms causing clotting deaths related to the COVID-19 spike mRNA shots not addressed by the CDC COVID-19 mRNA Safety Team of Dr. Sarah Meyer
One involves "bioweaponized SARS-CoV-2" (Image 4) , and one involves shedding of the mRNA spike protein on exosomes also referred to as "bioweaponized HERV-K102" (Image 3).

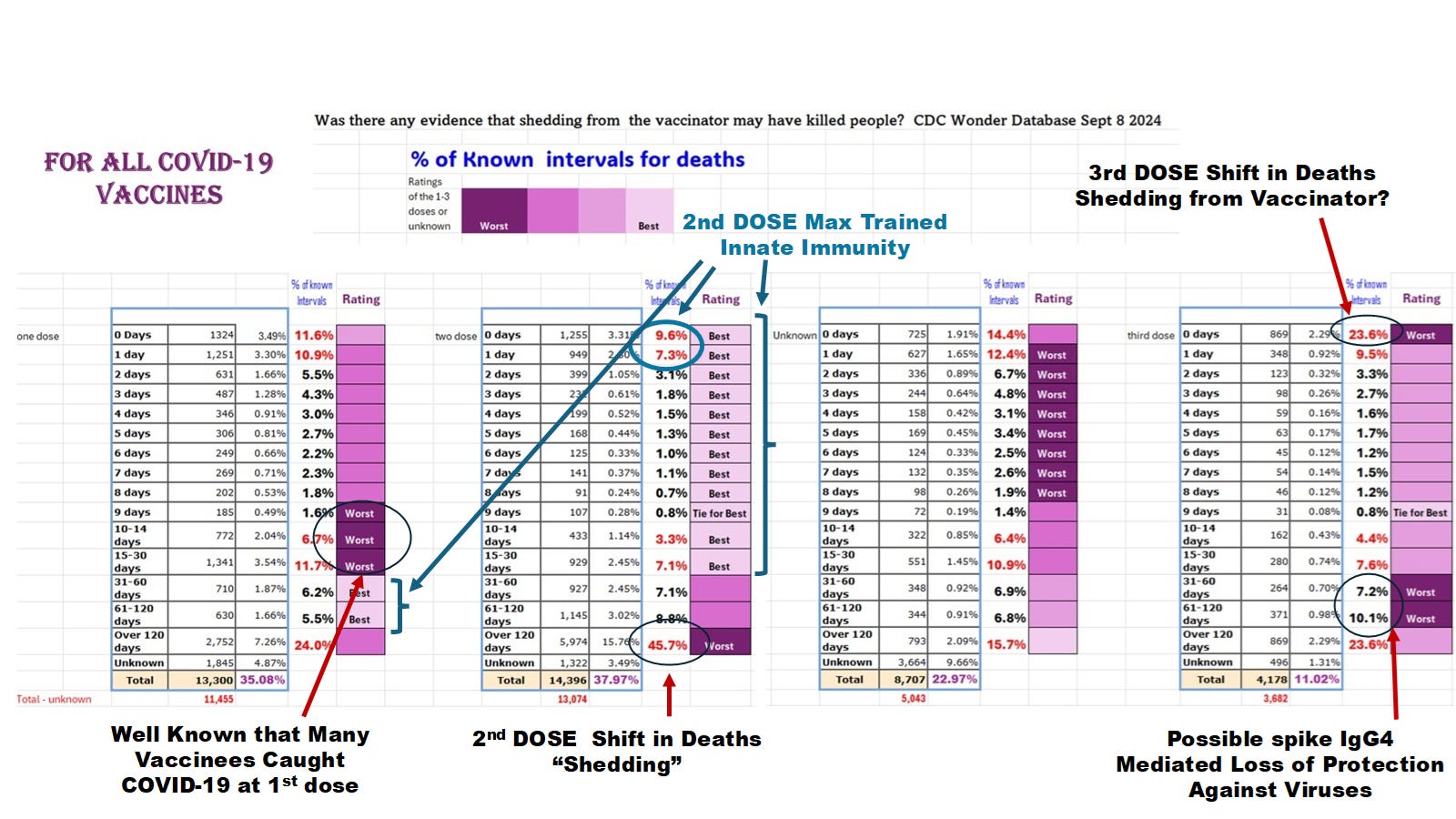
Image 1: Death Onset Intervals by Dose for the COVID-19 Vaccines.
As will be discussed below, the increased risk of deaths beyond 120 days referred here to as ”shedding” involves shedding deaths (Pfizer only) and/or bioweaponized SARS-CoV-2 infection (both the Pfizer and the Moderna mRNA gene therapy shots: see Image 4 below for definition/illustration of bioweaponized SARS-Cov-2).
Note, if the vaccinator was themselves recently injected with the third Pfizer dose (see third dose above for increased deaths within 0 days (23.6 % of all the deaths where the interval is known after the 3rd shot) compared with 2 doses (9.6 %) or one dose (11.6 %) then this data might suggest there could be shedding from the vaccinator as the general maximal levels of spike IgG1/3 would be in the upper respiratory tract (URT) of the vaccinator with dose 3 and in the blood circulation of the vaccinee.
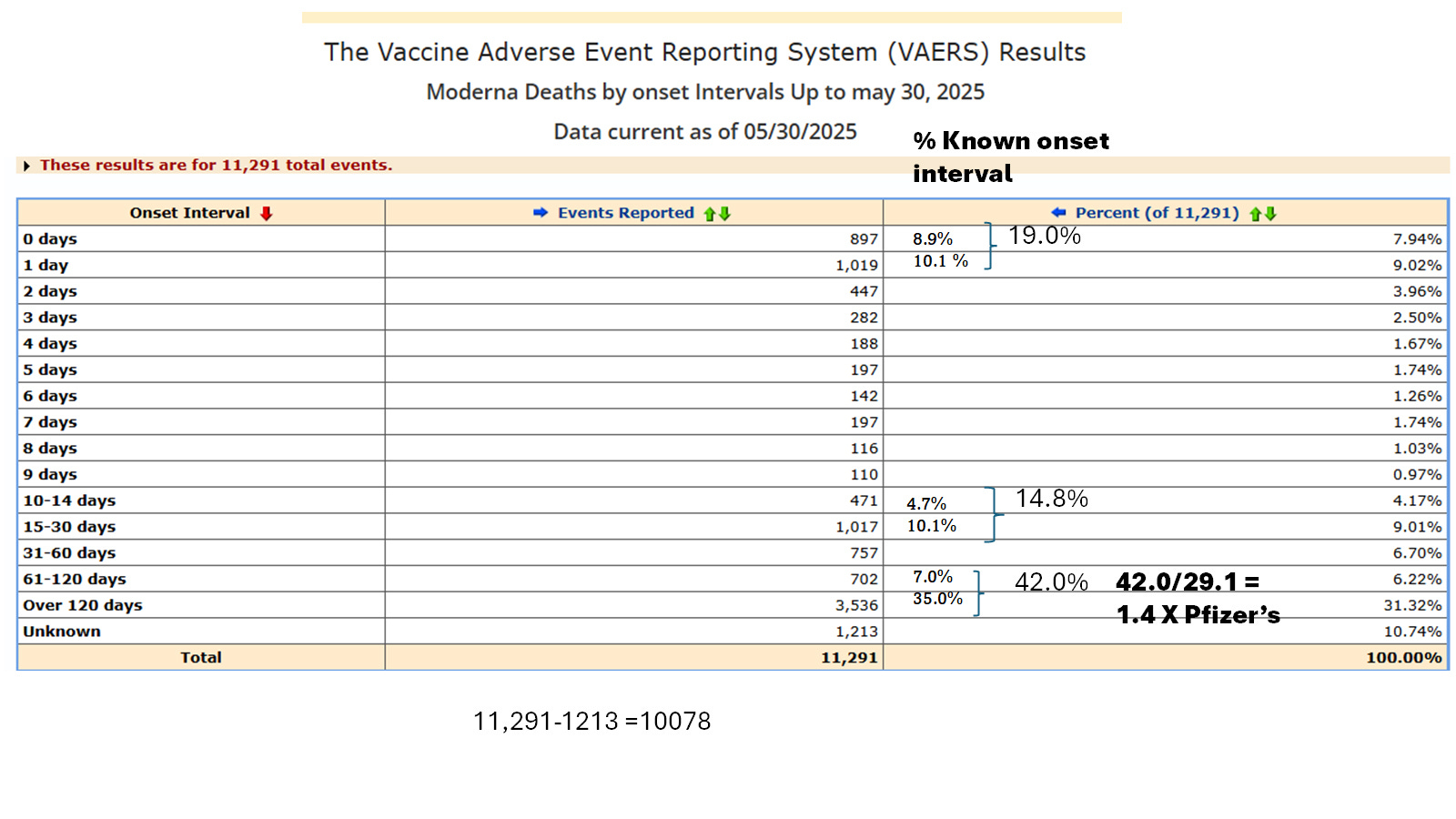
Image 1A. Day 0 death onset intervals for Moderna at 8.9 % of the total, is far less than that reported for Pfizer (17.5 % Image 1B) while the >60 day death onset intervals represent a higher % of the totals for Moderna verses Pfizer (42.0% vs 29.1 %). The Day 0 and day 1 for Moderna was 19.0% while for Pfizer it was 28.8 %.
Note since the mRNA does not express significant levels of spike protein until after day 2, it is possible that the high levels of deaths for Moderna for onset intervals covering 0 days and 1 day could be due to the vaccinator shedding (after they were recently immunized with the second or later doses of the Pfizer shots. Note as developed here only the dirty process 2 Pfizer shots are thought to shed.).
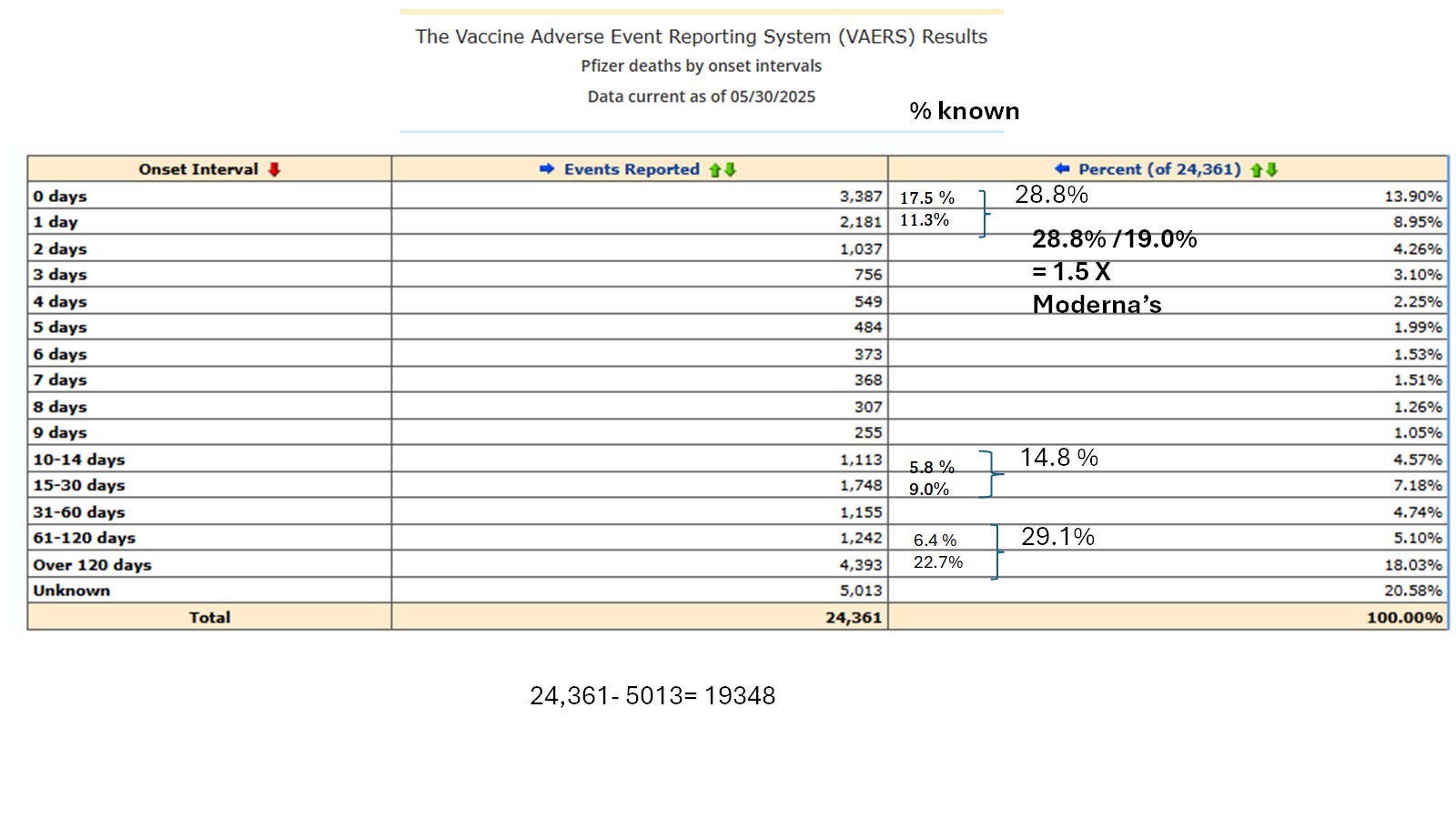
Image 1B. Pfizer Death Onset Intervals and % of Known Onsets.
The levels of Day 0 deaths was more pronounced in those receiving the Pfizer shots when compared with Moderna.
For a more concise overview on the two types of clots induced with the COVID-19 spike mRNA gene therapy shots (also colloquially referred to as the mRNA clot shots) please see: Laderoute MP. Two Types of Clots (NOVEL white rubbery with S protein and coffee ground like microclots). Surprise, Surprise... Two Clotting Mechanisms Proposed for the COVID-19 spike mRNA gene therapy CLOT SHOTS! July 7, 2025. https://x.com/hervk102/status/1942199206967451816.
Please note that I suggested only the Pfizer lipid nanoparticles (LNPS) could lead to shedding symptoms, injuries and deaths. This involved the generation of bioweaponized HERV-K102 that results from the dirty process 2 LNPs which does not occur with Moderna which appears to be from clean process 1 type PCR’d LNP. The shedding issues started around April 2021 in the USA (about 30 days after the second shots administered to the 70+) and when the delta variant was first being selected by the spike mRNA gene therapy products. At this time, the activity and spread of SARS-CoV-2 is very low in the community in part due to the heightened activity of innate immunity protection (see Image 1 above). As other ages are being vaccinated this keeps up the Pfizer shedding (and also as might be from the vaccinators at the clinics). Nevertheless by 120 days or 4 months, the levels of activity and dominance of the delta variant increases in the community, which now allows for the bioweaponized SARS-CoV-2 to cause injury and death for both the Moderna and Pfizer vaccinated. Nevertheless since other age groups are still being immunized the COVID-19 associated deaths are higher for Pfizer over Moderna during the first year of the vaccine rollout [Levi R et al, medRxiv 29 April 2025].
GROSS NEGLIGENCE BY THE CDC
In a recent ACIP meeting on June 25, 2025, Dr. Meyer (CDC Safety team for the COVID-19 spike mRNA shots) explained how they didn’t examine deaths beyond 42 days in their safety assessment of the COVID-19 mRNA gene therapy vaccines. However, as Dr. Robert Malone aptly pointed out, traditionally vaccines are monitored for up to 30 to 42 days when the antigen is known to clear from the host after a few days. However the antigen spike from the mRNA shots sticks around for up to 700 days meaning any deaths that occur between day 0 and day 742 should be considered possibly related to the COVID-19 mRNA shots.
Moreover due to the problem of antibody dependent enhancement (ADE) of infection into macrophages, following the selection of variants when adaptive immunity vaccines are used during active pandemics, one can expect to see a significant number of deaths with onset intervals well beyond 60 days (as was the case for both COVID-19 spike mRNA manufacturers (Image 1 and 1A and 1B).
I had a very hard time believing that Dr. Meyer had not looked at the complete repertoire of “onset intervals” for deaths such as represented in Image 1 by dose. In particular there are a very high number of deaths that occur beyond 60 days, especially beyond 120 days. You don’t see these deaths for traditional vaccines beyond 60 days unless you happen to be immunizing when the virus is actively being transmitted such as a pandemic (like for SARS-CoV-2) or an endemic virus like dengue. The subsequent increased risk of death commonly relates in part, to the problem of antibody dependent enhancement (ADE) of infection into macrophages making the subsequent infections with selected variants more deadly.
___________________________________
For more information on ADE and how being vaccinated when the virus is actively spreading can increase your subsequent risk of death upon reencounter, please see my recent review:
Published as a chapter in a medical book:
Laderoute MP. Chapter 17. Controversies Concerning the Immunology of the COVID-19 Adaptive Immunity Vaccines. In: Controversies in the Pandemic. Ed(s); J Varon, PE Marik, M Rendell, J Iglesias, C de Souza, P Prabhudesai. Jaypee Brothers Medical Publishers Ltd, New Delhi, India, 2024, pp 760. ISBN: 978-93-5696-730-4.
But also available for free downloading here:
Laderoute, M. Antibody Dependent Enhancement (ADE) of Infection into Macrophages Validates the Importance of HERV-K102 Particle Production for Pandemic Preparedness. Preprints 2023, 2023120185. https://www.preprints.org/manuscript/202312.0185/v2.DOI: 10.20944/preprints202312.0185.v2.
________________________________________________________
But these mRNA shots are very novel, and one thing that they do that remains largely unappreciated is that they ABNORMALLY cause high levels of spike IgG1 and IgG3 in the upper respiratory tract [Roubidoux EK et al, Science Reports, 2023]; ESPECIALLY IN INDIVIDUALS WHO WERE INFECTED WITH SARS-COV-2 BEFORE VACCINATION [Sano K et al, Nature Communications 2022]. There were some reports that Moderna which had twice the concentration of mRNA than Pfizer provided the highest increase in intranasal antibodies and displayed higher neutralizing capacity [Cao KT et al, J Allergy Clin Immunol Glob, 2023]. Generally health care workers, younger adults (18-29) or children were at higher risk of being infected prior to receiving the mRNA gene therapy shots (the last two groups because they were immunized later than the rest of the population). In these individuals who were infected before receiving the spike mRNA gene therapy products, there was no conversion of spike IgG1/3 (complement binding) in the blood to non-complement binding IgG4 [Irrgang P et al, Science Immunology 2022]. This means should there be a subsequent transmission of SARS-CoV-2 or worse a complex of SARS-CoV-2 with the spike IgG1/3, these individuals would be at a higher risk of dying due to higher levels of complement binding IgG1/3.
Not surprisingly, Moderna with a higher concentration of mRNA was found to be more apt to cause higher levels of these complement binding antibodies as reported by many but not all investigators. Apparently, substantial increases in sIgA in saliva or nasal secretions upon mRNA vaccination occurs in those who were naturally infected before vaccination and where Moderna generated more antibody to spike protein (IgA and IgG) than Pfizer in blood and saliva [Gorochov G et al, JAMA Netw Open April 2024]. However others have reported while Moderna mRNA shots induced higher antibody levels in nasal secretions there were no difference in antibody levels in serum when Pfizer and Moderna are compared [Cao KT et al, J. Allergy Clin Immunol Glob June 25, 2023]. Serrano L et al in a study of health care workers [J. Appl. Microbiol, September 2022] reported almost double the amount of antibody in blood in response to Moderna mRNA shots over Pfizer and again those with previous infection exhibited significantly higher levels of spike antibodies in blood.
We don’t know for sure how the Moderna vaccine was made if it used clean process 1 or dirty process 2 for the manufacture of the lipid nanoparticles (LNPs) as described by Pfizer (Image 2). If it was made by PCR (similar to the CLEAN process 1 for Pfizer), then it would lack spike protein and would not contain high levels of endotoxin from E. coli (dirty process 2). If that is the case then one might expect very little or NO shedding from the Moderna vaccinated and generally lower toxicity.
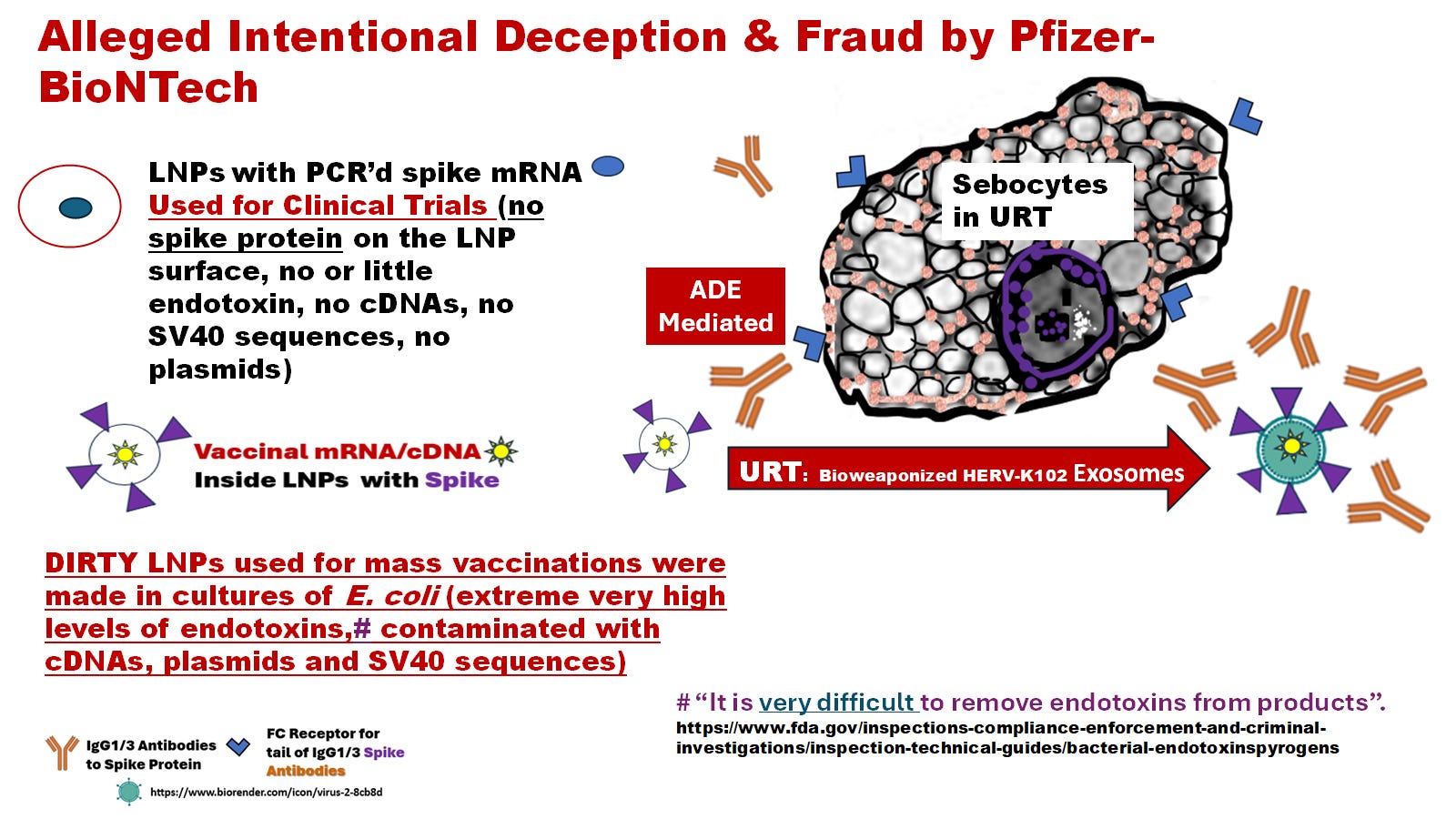
Image 2. Pfizer used clean preparations of the mRNA encapsulated in LNPs for clinical trials (process 1), but deployed dirty preparations (process 2) for injection into the masses.
As will be discussed only the dirty Pfizer LNPs covered in spike protein, are capable of being shed. Moderna apparently only used PCR (similar to Pfizer’s clean process 1) and so is believed not to cause shedding. Presently we do not know if the shed particles (compromised HERV-K102 foamy retrovirus particles referred to as CD9 positive exosomes in the literature ) carry the spike mRNA of Pfizer-BioNTech. We do know they carry high levels of at least S2 protein [Bansal S et al, J Immunol 2021]. If the shed particles carry spike mRNA, then the risk of integration into the genome of the new host is much higher because we know HERV-K102 is replication competent and can undergo increased integration [Laderoute M et al, Open AIDS J, 2015]. As a functional protector foamy retrovirus it carries its own reverse transcriptase and integrase. If any of the integrated spike sequences start with “tgtg” then we know it used the integrase of HERV-K102. The line 1 elementS use a recognition sequence of CTTT/A, TTTT/A OR TTTT/C [Zhang L et al, PNAS May 6, 2021.]
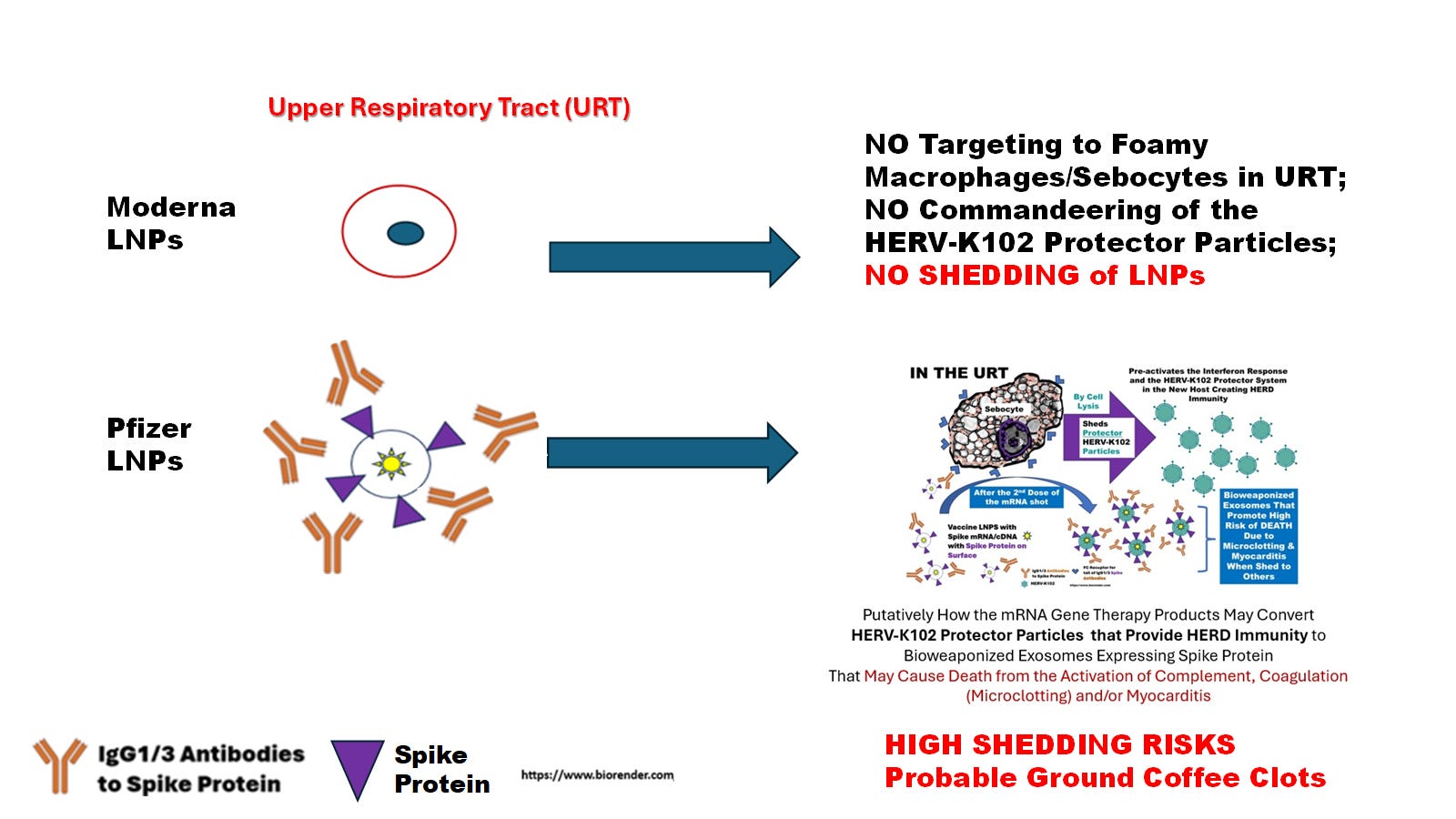
Image 3. Moderna apparently only used PCR (similar to Pfizer CLEAN process 1) and so is believed to NOT cause shedding.
As will be discussed, the recent preprint by Levi R et al., [medRxiv April 29, 2025] concerning Florida residents, and the 12 months following the second dose of either Pfizer’s BNT162b2 compared with matched Moderna’ mRNA-1273 recipients (including census tract), it was demonstrated that the risk of deaths (all-cause, cardiovascular, COVID-19 and non-COVID-19 mortality) were significantly elevated for recipients of the Pfizer shots despite the fact that the Moderna shots contained twice the amount of mRNA. Note that it is thought shedding along with the bioweaponized SARS-CoV-2 transmission, would increase the risk of COVID-19 deaths in recipients of BNT162b2 when compared with ONLY the bioweaponized SARS-CoV-2 transmitted from Moderna spike mRNA exposures. Of course for Pfizer, both shedding and transmission of the bioweaponized SARS-CoV-2 could happen at the same time, increasing the risk of death to the unfortunate recipient.
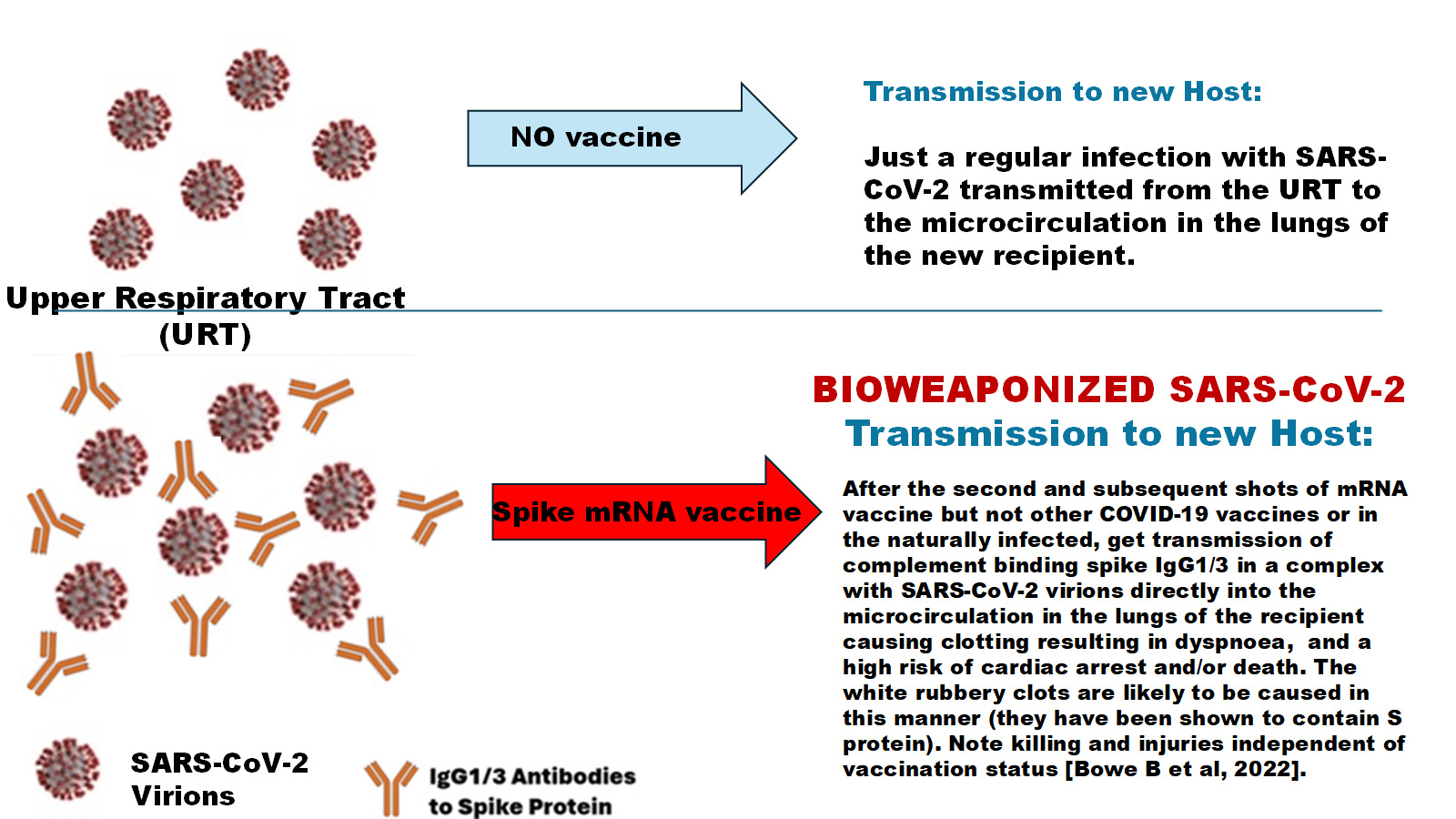
Image 4. Bioweaponization of SARS-CoV-2 Refers to SARS-CoV-2 Transmitted from the Upper Respiratory Tract (URT) to a New Host with “Bound Spike IgG1/3 after the second and subsequent doses of COVID-19 spike mRNA gene therapy shots”.
The Cleveland Clinic data suggests in the URT there is no conversion of spike IgG1/3 to IgG4, just higher levels of IgG1/3 antibodies made [Shrestha NK et al, Clin Infect Dis, 2022]. The transmitted complex of SARS-CoV-2 with the complement binding spike IgG1/3 likely triggers clotting upon reaching the microcirculation deep in the lungs of the recipient. It may be more dangerous than shedding because 1) shedding might only involve S2 and not S1 determinants [Bansal S et al, J. Immunol , 2021], and 2) the density of epitopes on the SARS-CoV-2 particles may be higher and thus more efficient at complement binding. On the other hand, for people who were infected before vaccination, they may have more antibodies to S2, and thus, at higher risk of shedding causing death/injury. One might consider that the main reason delta was more lethal than any of the other variants is that it was commonly transmitted with the deadly spike IgG1/3 antibodies. NOTE: people infected before vaccination are more likely to not convert the spike IgG1/3 in blood to IgG4, and thus, are at much higher risk of clotting/microclotting.
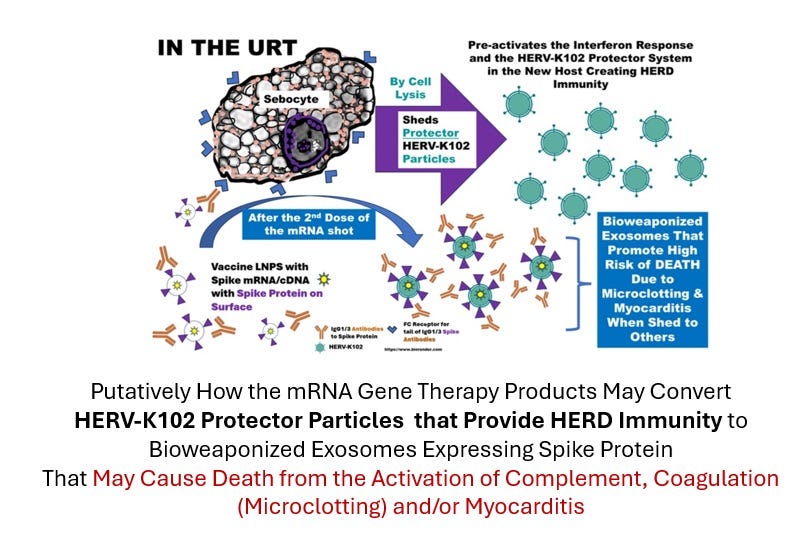
Image 5. Pfizer’s Dirty LNPs covered in Spike Protein would be targeted to the Sebocytes (specialized foamy macrophages in sebaceous glands that line the mucosa) and then shed as S2 covered CD9 exosomes [Bansal S et al, J Immunol, 2021] (thought to be commandeered HERV-K102 particles).
NB: We do NOT know if spike mRNA is also shed.

Image 6. Table of Onset Intervals for Deaths Following the Second Dose of Moderna or Pfizer/BioNTech.
By listing the onset intervals following the second dose, it allows us to zoom in during the time frames when death was first related to the development of the spike antibodies after the second dose. At all onset intervals the Pfizer vaccine causes a higher percentage of deaths except for beyond 120 days where for Moderna the 2,663 deaths represented 57.9% of the known onset intervals (for Moderna) and for Pfizer at >120 days it was 3345 deaths or 39.43% of the known onset intervals for Pfizer. This is consistent with the notion that Pfizer was more toxic due to impurities and/or following the second dose, Pfizer shots caused shedding increasing death risks whereas Moderna apparently did not.
It should also be noted that the deaths for Moderna after the second dose for day 0 and day 1 were 11.2 % of the total whereas for Pfizer it was 19.8 % (about 1.77 fold higher). It is possible that the people vaccinating the masses may have been recently vaccinated themselves. If vaccinated with Pfizer, this could lead to shedding onto the vaccinees. Because Pfizer dominated the immunization campaign it is possible that some of the vaccinators even for the Moderna vaccines had been recently vaccinated with Pfizer shots.
Image 7. Inversion with the Third DOSE. With Dose 3 we generally see that Moderna causes higher % deaths at all onset intervals EXCEPT day 0. This contrasts with Image 6 where Pfizer generally shows a higher % of the total for most of the death onset intervals after the second dose. The meaning of this inversion remains unclear but possibly it reflects fewer Pfizer vaccines being administered and/or that Moderna has been shown to increase antibody production over Pfizer due to higher concentrations of mRNA (and it is the spike antibodies that are causing all the pathology).
If we looked at just the second dose or all doses together, the peak months for deaths was April 2021 (putative peak shedding episodes involving bioweaponized HERV-K102), August/September (putative peak bioweaponized SARS-CoV-2) and then January 2022 (Omicron with a complicated mix of some shedding and some bioweaponized SARS-CoV-2 as determined by symptoms mined from VAERS (data not shown).
In England the shedding deaths peaked in May, June and July of 2021 and disappeared by September 2021 (peaks last only 3-4 months upon vaccination with each dose but shedding only starts with the second dose related to the advent of the spike IgG1/3 [see Bansal S et al., J Immunology, 2021].
If we look at results for England for shedding deaths using a novel surrogate marker (non-COVID-19 death rates per 100,000 person years over COVID-19 death rates per 100,000 person years) we saw this image:
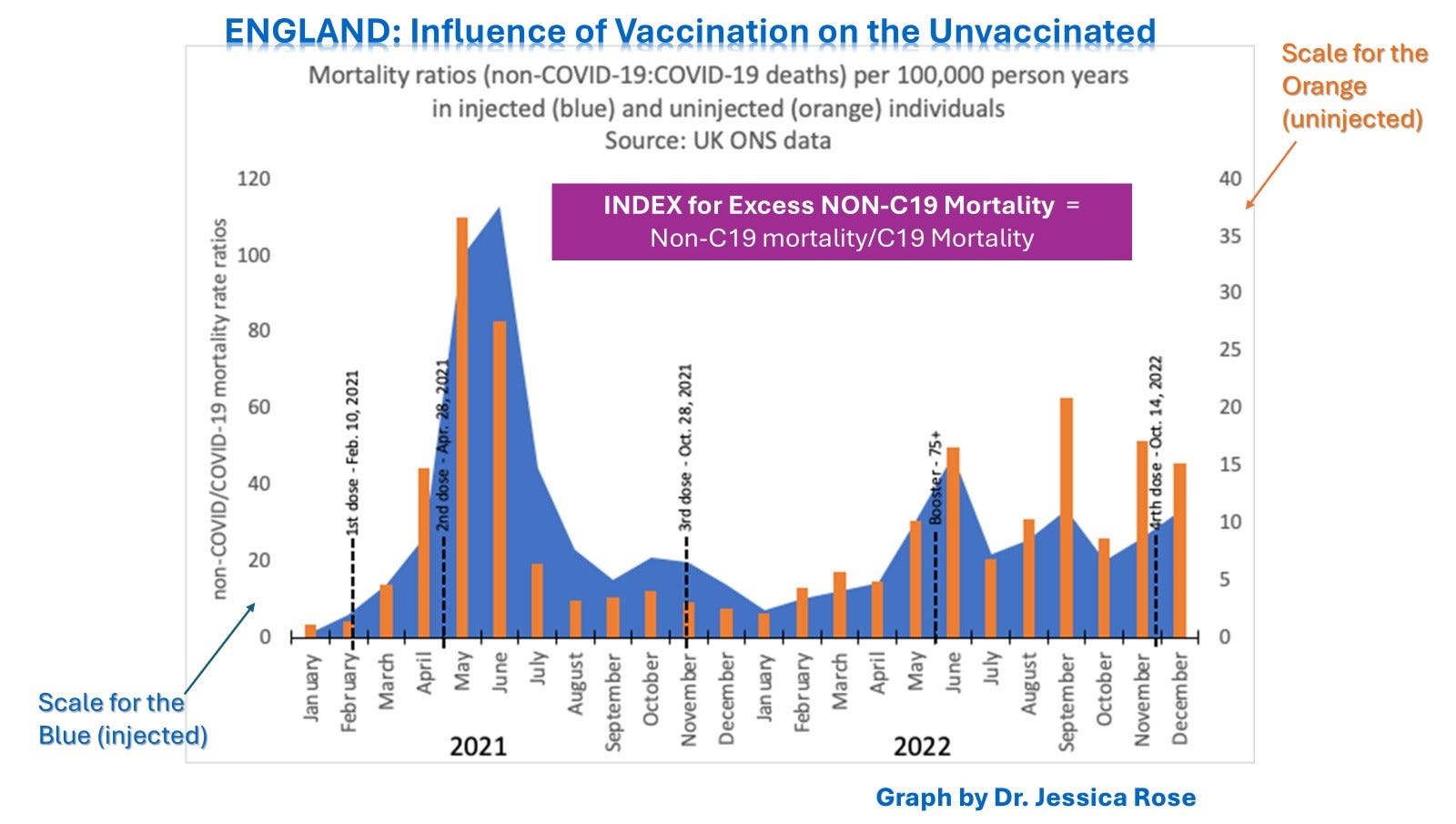
Image 8. Shedding was maximal after the second dose, all shedding episodes lasted 3 to 4 months and shedding affected the non-vaccinated. [From https://rumble.com/v51idm2-dr.-marian-laderoute-jun-01-2024-regina-saskatchewan.html]
But in the USA which did not delay the second dose, instead of the major shedding peak in May/ June/July 2021 for England, in the USA it was March/April 2021.
If we instead plot the inverse (COVID-19 mortality rates over the non-COVID-19 mortality rates) by vaccination status, we see in England that in August/September 2021 we get a peak after the initial peak in January 2021. We also get another larger peak in January 2022 but this involves Omicron which as mentioned complicates things.
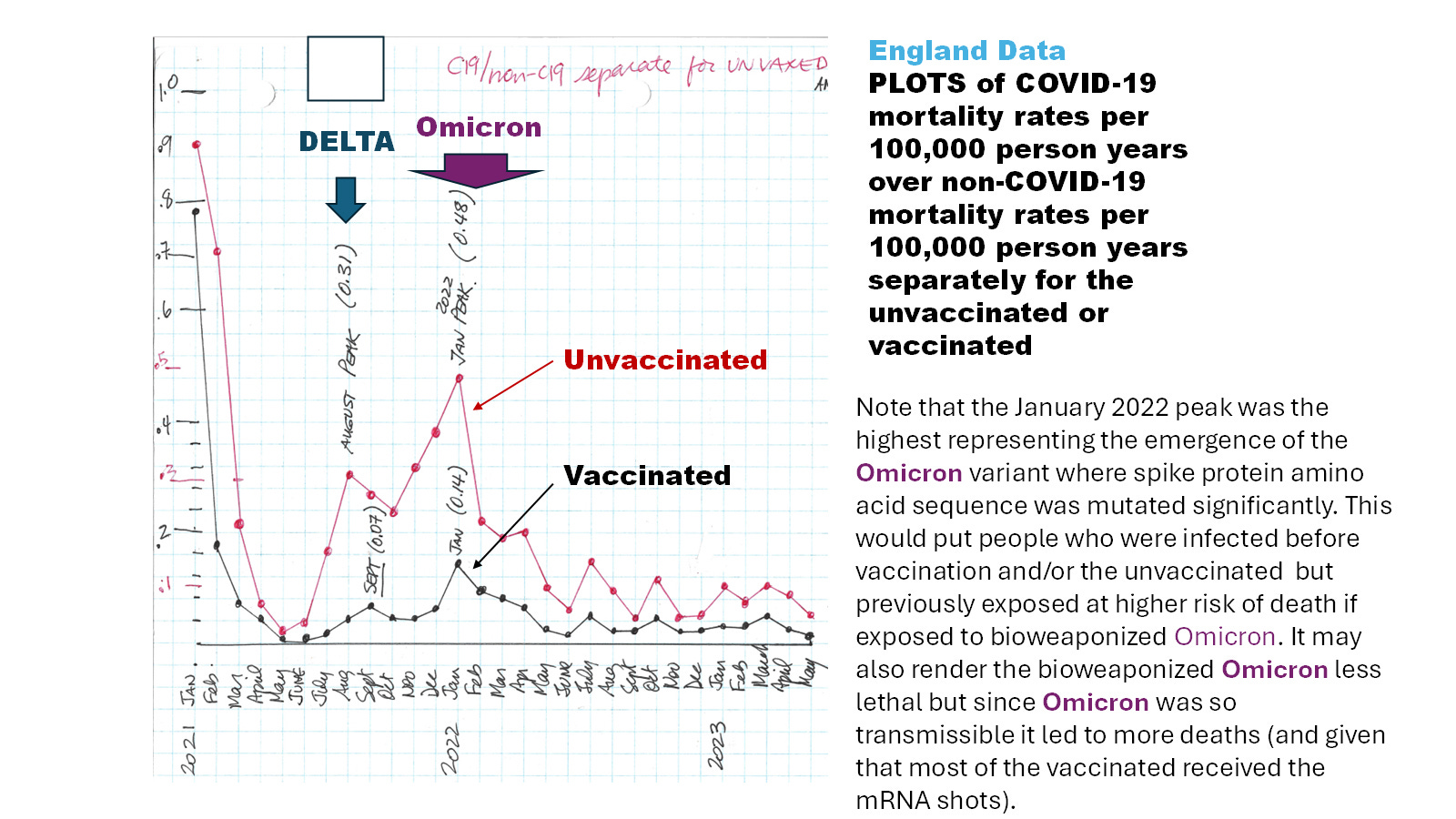
Image 9. Bioweaponized SARS-CoV-2 (bwSC2) Led to more deaths July 2021 to April 2022 in England in the unvaccinated with peaks in August-September 2021 (Delta) and January 2022 (Omicron).
The vaccinated without a previous infection would be at a lower risk of dying from bwSC2 than those with a previous infection.
Image 9 plots the COVID-19 death rates over the non-COVID-19 death rates so the vaccinated who had way more non-COVID-19 deaths than the unvaccinated, lowers the COVID-19 death rates over the non-COVID-19 death rates ratio. These peaks seem to portray the bioweaponized SARS-CoV-2 deaths and tell us when they were most common.
Overall, the clotting injuries and death would occur independent of COVID-19 severity risk factors and vaccination status (as was found by Bowe B et al, 2022). These severity risk factors instead pertain to the condition of the host immune system, such as age, hypertension, type 2 diabetes, cardiovascular disease, cancer and other chronic diseases. In fact these factors relate to a compromised trained innate immunity [for more info on trained innate immunity see Laderoute MP. Trained Innate Immunity: Mechanisms and Meaning. https://hervk102.substack.com/p/trained-innate-immunity-mechanisms]. No vaccine or monoclonal antibody (ie no active or passive immunization tool) is capable of preventing these deaths. They are clotting deaths and only anti-clotting therapies would help.
Bearing in mind that there are two types of clotting as described by the embalmers: the white calamari like rubber clots (likely evidence of bioweaponized SARS-CoV-2) and the ground coffee type clots (likely evidence of microclotting associated with shedding).
Below in Image 10, this is what was found by Bowe B et al, and reported in Nature Medicine in November 2022. For people who had a SARS-CoV-2 infection in 2020, then either vaccinated or not and experienced a breakthrough infection or re-infection (respectively) their risk of death was 1/100, hospitalization was 1/14.3 and experiencing a long term health issue was 1/4.
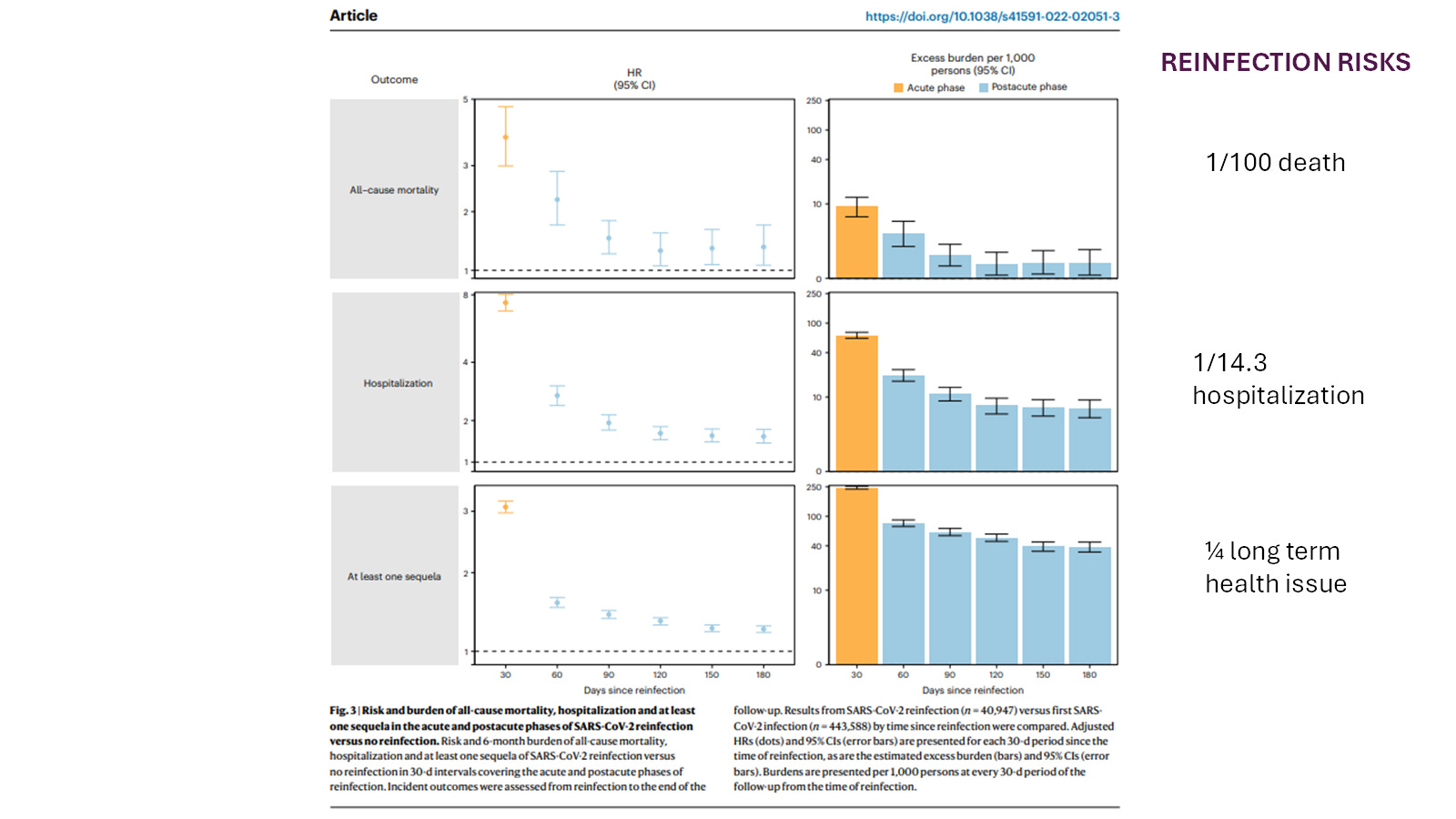
Image 10. Reinfection/breakthrough infections are incredibly dangerous associated with the mRNA technology. The strong induction of complement binding IgG1/3 spike antibodies in the URT which apparently transmit with SARS-CoV-2 putatively as a complex after the second dose is how SARS-CoV-2 becomes bioweaponized. That antibodies to spike protein are transmitted from the URT via aerosols has been shown by Kedl RM et al., Immunohorizons, May 1, 2023.
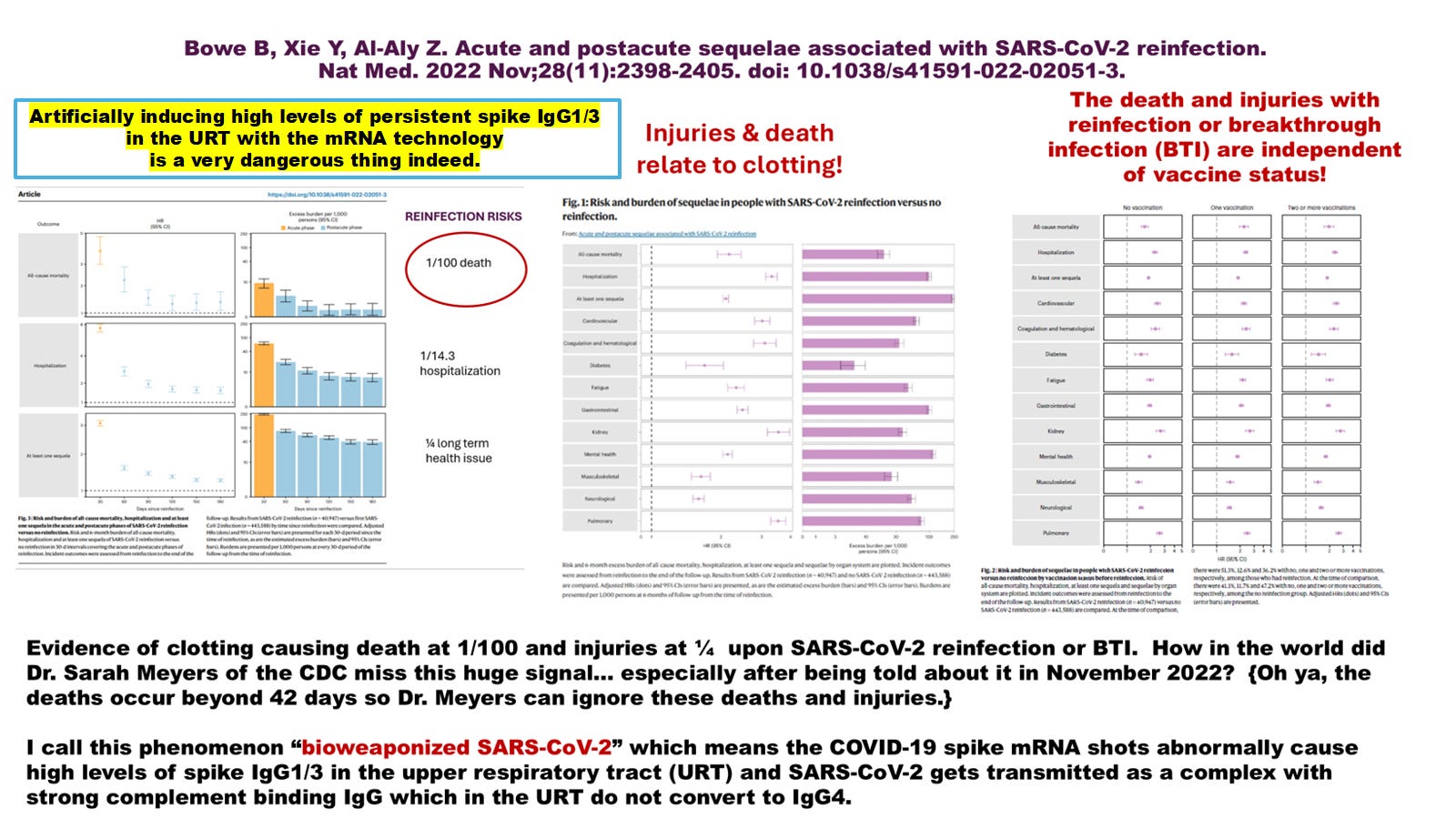
Image 11. Risk of severe consequences of re-infection with or without COVID-19 vaccinations when bioweaponized SARS-COV-2 is involved is unacceptable.
Note that the traditional risk factors for severe disease do not apply here, and elevated risk is independent of vaccination status.
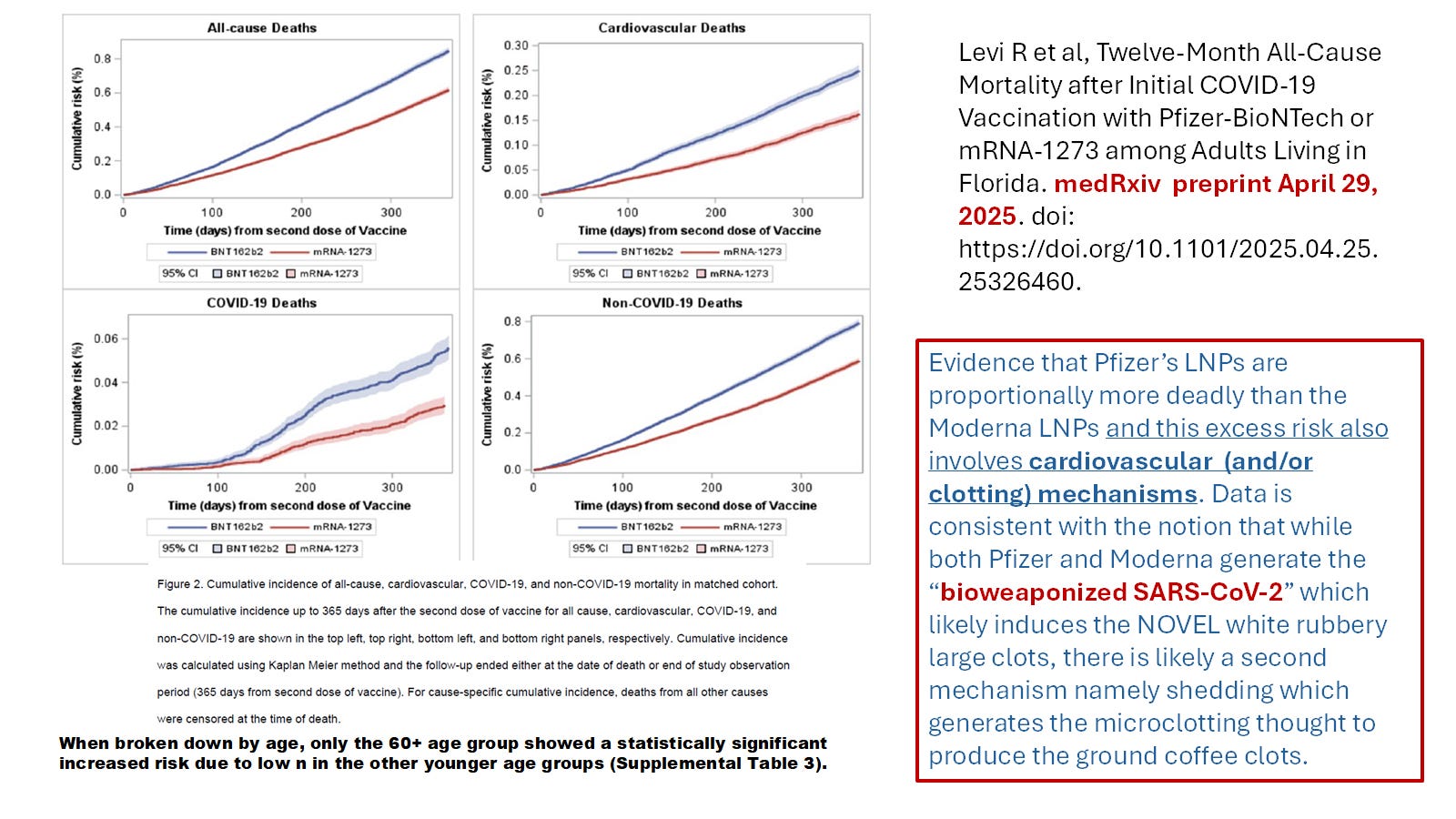
Image 12. Using matched cohorts in the Florida database for residents, Levi R et al, showed that there was an enhanced risk of death associated with the Pfizer vaccine over the Moderna for the first 12 months after the second dose (see Image 6 above). The finding of a dramatic jump around day 200 for the plot of Pfizer vs Moderna COVID-19 deaths implied to the authors that there may be at least two distinct mechanisms causing clotting/cardiovascular deaths with the Pfizer shot when compared with Moderna.
For more discussion on the Levi et al, paper please see:
Laderoute MP. Two Types of Clots (NOVEL white rubbery with S protein and coffee ground like microclots). Surprise, Surprise... Two Clotting Mechanisms Proposed for the COVID-19 spike mRNA gene therapy CLOT SHOTS! July 7, 2025. https://x.com/hervk102/status/1942199206967451816
Finally there are some differences in the symptoms that could help determine the proportion of deaths such as recorded in VAERS related to bioweaponized SARS-CoV-2 versus bioweaponized HERV-K102 and they are captured in Image 13 below.
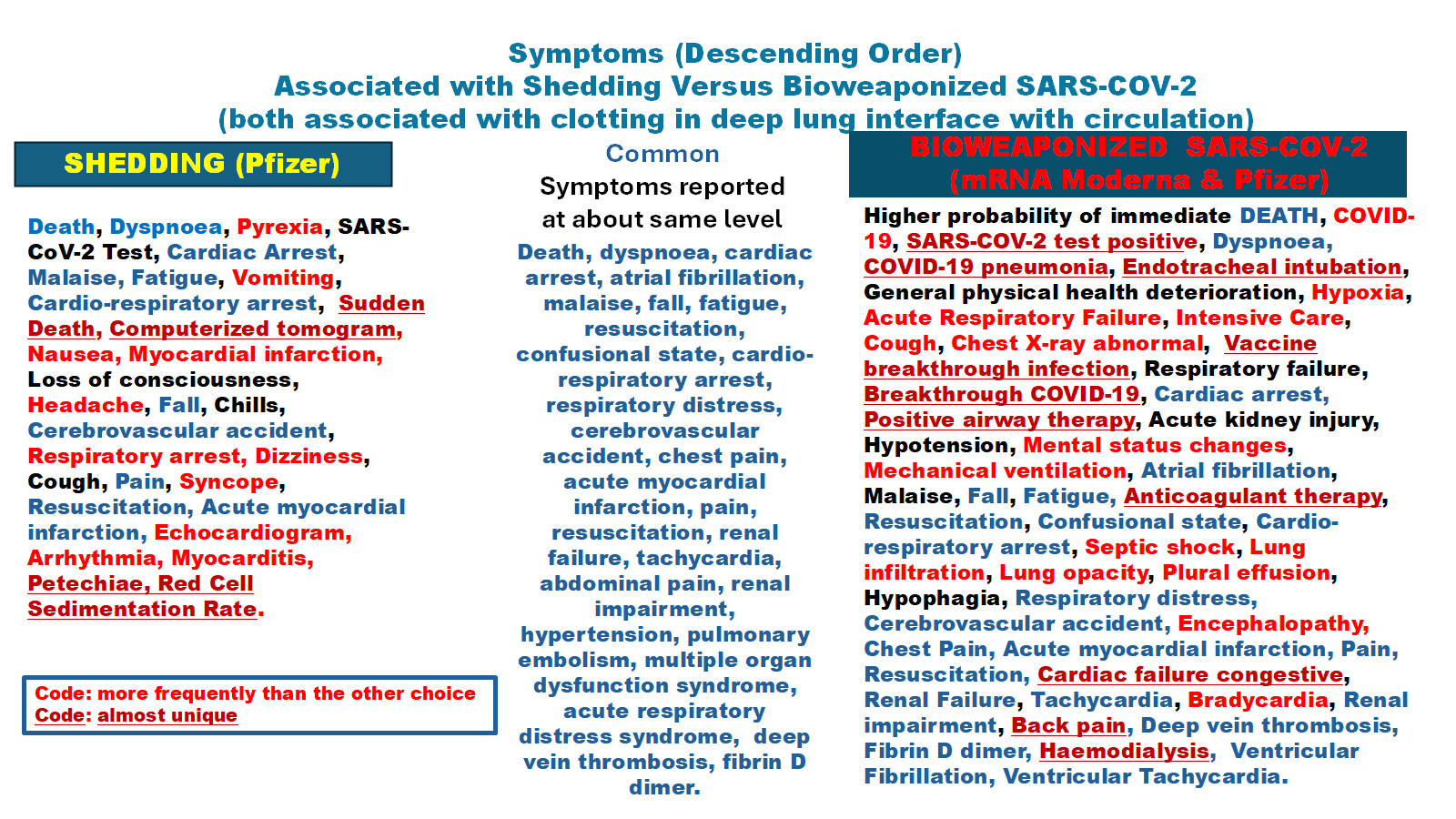
Image 13. For the clinician certain symptoms may be more frequent with clotting due to shedding while others particularly the involvement of SARS-CoV-2 or a clinical diagnosis of COVID-19 would indicate clotting by “bioweaponized SARS-CoV-2”. It is also possible that one individual could have both mechanisms of clotting at play. Generally the “bioweaponized SARS-CoV-2” is more likely to result in death (or the inability to resuscitate?). Presumably the involved spike protein would be the Pfizer sequence for all shedding cases (which currently the evidence suggests is the S2 protein) while the bioweaponized SARS-CoV-2 would carry the full spike sequence of whatever variant is involved. Clearly more research is needed.
SUMMARY
In this paper I have attempted to rationalize how and why embalmers saw completely NOVEL white rubbery clots starting in mid 2021 in the USA (bioweaponized SARS-CoV-2) and also found evidence of microclotting (otherwise rare), in association with the (inappropropriate) deployment of the COVID-19 spike mRNA gene therapy technology by the FDA/CDC. The EUA process lacked any consideration of the novel risks and inherent dangers of this technology and the problems with adaptive immunity vaccination (ie. ADE see Footnote 1 below) during an active pandemic. Worse the shedding and integration studies that are usually required for a gene therapy product were ignored and not performed before or after the EUA (to the best of my knowledge).
Even years later the CDC (June 25, 2025) and even GROK3 (July 7, 2025 on X) refuse to admit the spike mRNA gene therapy clot shots caused significant levels of injuries and deaths related to the bioweaponization of SARS-CoV-2 and also the bioweaponization of the protector foamy retrovirus of humans HERV-K102. If the ACIP panel members do not know anything about how the protector HERV-K102 foamy retroviruses generate trained innate immunity that provides heterologous protection against all-cause mortality and how this is accomplished and interred with by adaptive immunity vaccines, they can read about it here:
Laderoute MP. Trained Innate Immunity: Mechanisms and Meaning. https://hervk102.substack.com/p/trained-innate-immunity-mechanisms
The issue of the Pfizer vaccine causing shedding is discussed here;
Laderoute MP. Shedding of Spike mRNA "Gene Therapy Products": Potential Mechanisms and Mortality Outcomes. Sworn Testimony to the National Citizen’s Inquiry, June 1, 2024.
https://rumble.com/v51idm2-dr.-marian-laderoute-jun-01-2024-regina-saskatchewan.html
And to get an understanding of the impact of shedding in England during the first 17 months of the Pfizer mRNA shot roll out I have summarized the statistics below in Image 13.
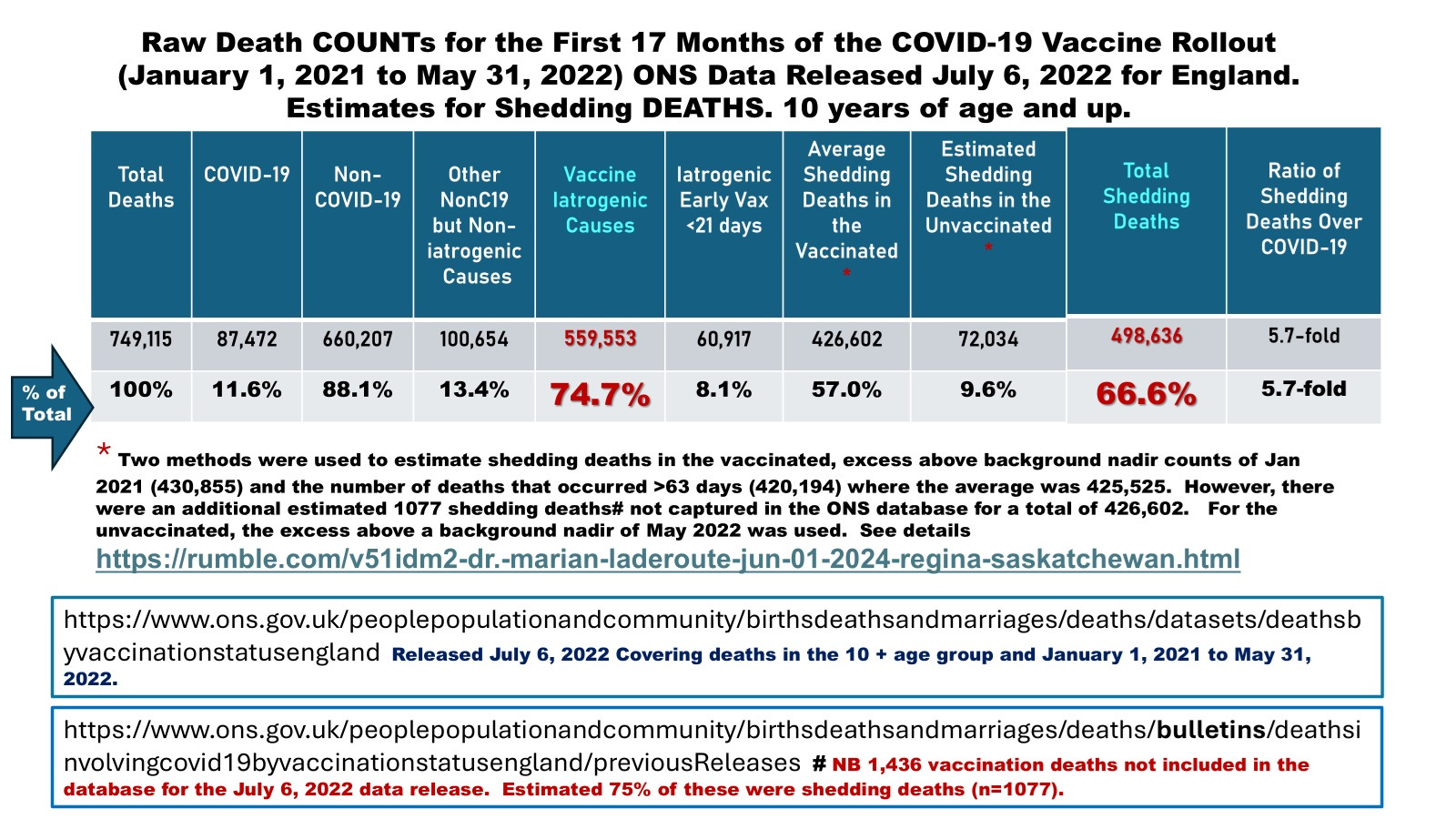
Image 14. In England where the Pfizer COVID-19 mRNA gene therapy product was predominately used, we can see based on raw death counts that shedding was the most common cause of death during this period.
In CONCLUSION
The big surprise here is that for the most part, the “CLOT SHOT” problems of the mRNA gene therapy shots causing clots relates to the abnormal generation of high levels of spike IgG1/3 in the URT (LNPs DO NOT STAY IN THE ARM, SO THEY HARM).
I suppose now we know NOT to approve or RECOMMEND any vaccine that causes high levels of pathogen specific antibodies in the URT.
HOW ABOUT CUTTING TO THE CHASE by immediately banning the use of gene therapy technology for immunization purposes in humans, animals and plants including their study in animals, and in clinical trials. This ban should clearly also apply to the upcoming cancer treatment and prevention vaccines AND VACCINES USED FOR ANY OTHER PURPOSE.
I would still favor the CDC linking the vaccination record to the mortality database so that relevant information on shedding raw numbers (Image 13), the impact of shedding on the vaccinated and unvaccinated (Image 8), the impact of bioweaponized SARS-CoV-2 on the unvaccinated (Image 9) and the true risks and benefits of the mRNA clot shots on reducing the risks of deaths can be clearly ascertained as shown here for England (Image 14).
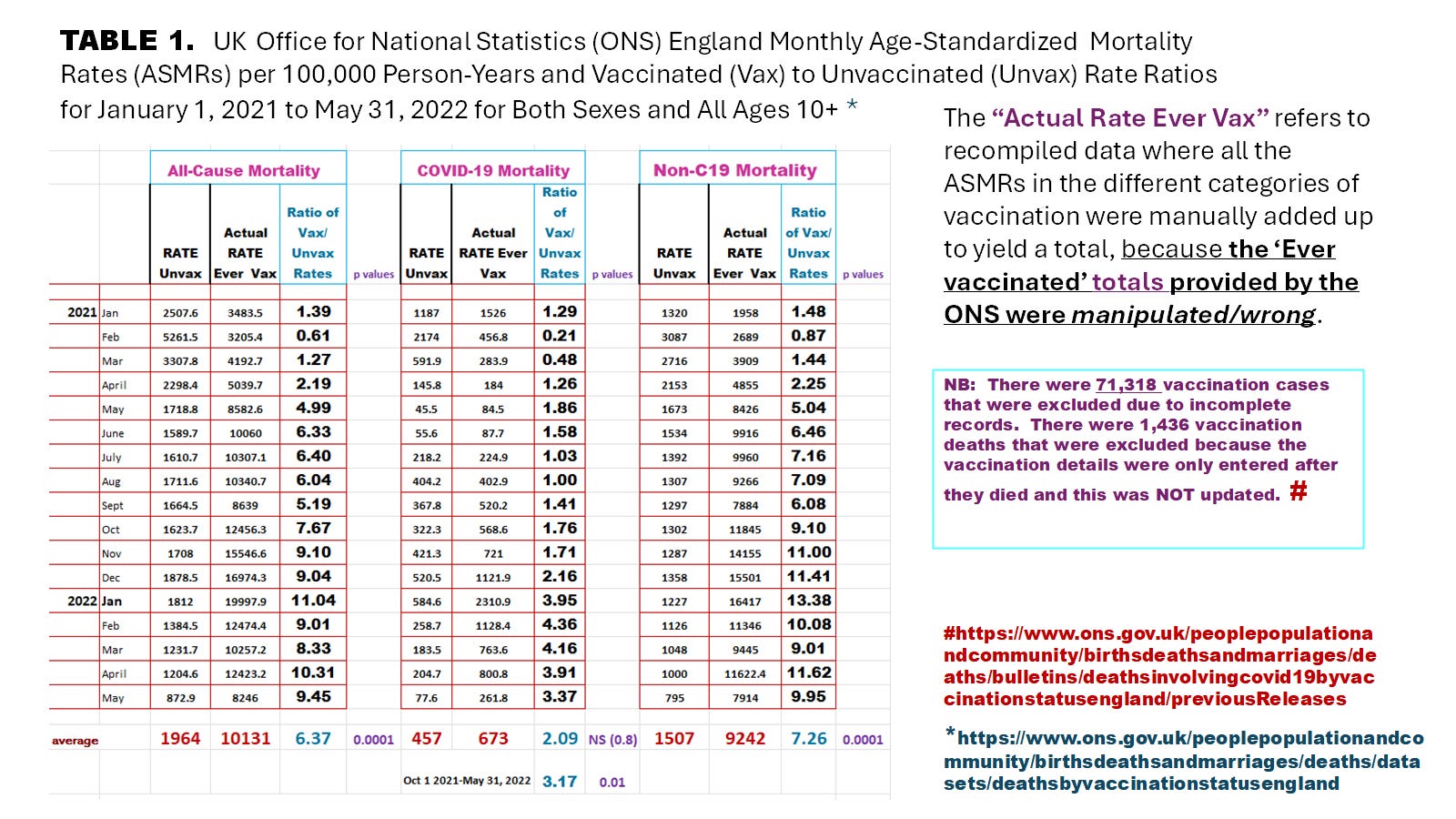
IMAGE 15. A comparison of mortality rates per 100,000 person years in the vaccinated when compared with the unvaccinated shows how grossly unbalanced the risks were that worsened over time in the vaccinated.
________________________________________
Footnote 1. YOU CAN READ MORE ABOUT THIS IMPORTANT TOPIC OF HERV-K102 PARTICLE PRODUCTION IN FOAMY MACROPHAGES HERE:
Published as a chapter in a medical book:
Laderoute MP. Chapter 17. Controversies Concerning the Immunology of the COVID-19 Adaptive Immunity Vaccines. In: Controversies in the Pandemic. Ed(s); J Varon, PE Marik, M Rendell, J Iglesias, C de Souza, P Prabhudesai. Jaypee Brothers Medical Publishers Ltd, New Delhi, India, 2024, pp 760. ISBN: 978-93-5696-730-4.
But also available for free downloading here:
Laderoute, M. Antibody Dependent Enhancement (ADE) of Infection into Macrophages Validates the Importance of HERV-K102 Particle Production for Pandemic Preparedness. Preprints 2023, 2023120185. https://www.preprints.org/manuscript/202312.0185/v2.DOI: 10.20944/preprints202312.0185.v2.
In the first place, organisms basically do not use mRNAs with methylated Uridines.
The platform that uses this methylated Uridine is incorrect.
Kariko is a crime of unfortunate murder.
Thank You, Dr. Laderoute, for keeping up the fine work.
I will excerpt this and link to it in my next blog post.