

The New Rule: Under 50% VE (Vaccine Effectiveness) Could be Associated with an Absolute Increase in Infections, Hospitalizations and/or Deaths
The New Rule: Under 50% VE (Vaccine Effectiveness) Could be Associated with an Absolute Increase in Infections, Hospitalizations and/or Deaths
March 29, 2022

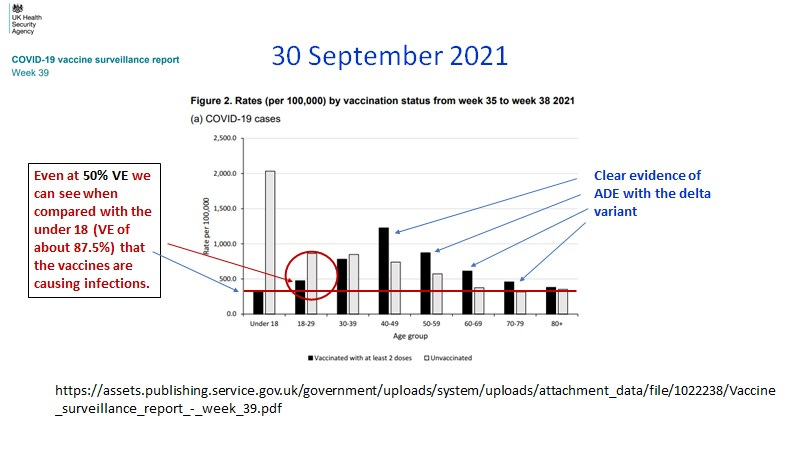
Image 1. Explanation of how VEs less than 50% (a relative metric) could be associated with an absolute increase in infections.
In Image 1 taken from published data by the UKHSA is shown how vaccine effectiveness under 50% could still be associated with an absolute increase in infections per 100,000.
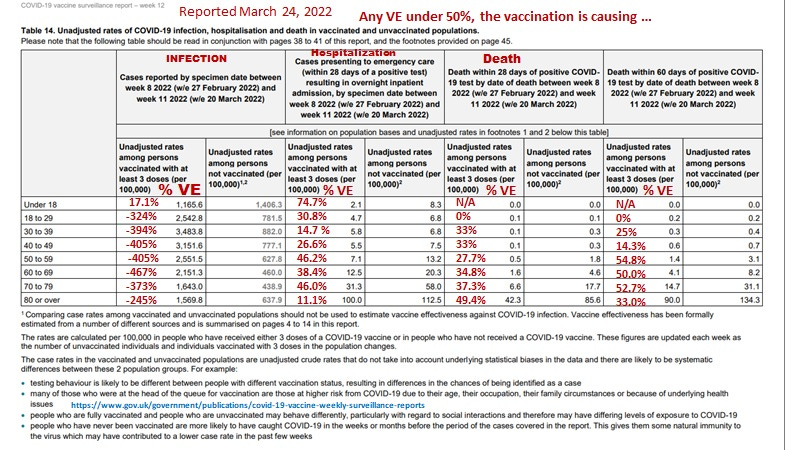
Image 2. An interpretation using the 50% rule of the most recent data from the UKHSA reveals with few exceptions, the 3 dose vaccination protocol may be promoting infections, hospitalizations and deaths associated with the Omicron variant.
Using the new rule of VEs under 50% we see for the latest data from the UK (Image 2) that 3 doses of vaccine are strongly promoting infections, as well could be causing increases in hospitalizations and deaths involving the Omicron variant.
While the negative VE for symptomatic infection is obvious from the numbers (ie., vaccinations are highly promoting infection probably by ADE), substantiation of the notion that vaccination may promote Omicron hospitalization and deaths is less obvious. Accordingly, the latter two are confirmed in Images 3 and 4 with UK specific data, albeit, the increased peak risk is in part explained by the shortened duration of the peak.
That the duration of the peak has been shortened might be an argument that Omicron infection may promote (innate immunity) sterilizing immunity which diminishes spread/reinfection/breakthrough infections. However, spike mRNA booster shots would be expected to lower this benefit. Both hospitalizations and mortality (Images 3 and 4) show an uptick potentially related to stealth Omicron (BA.2).
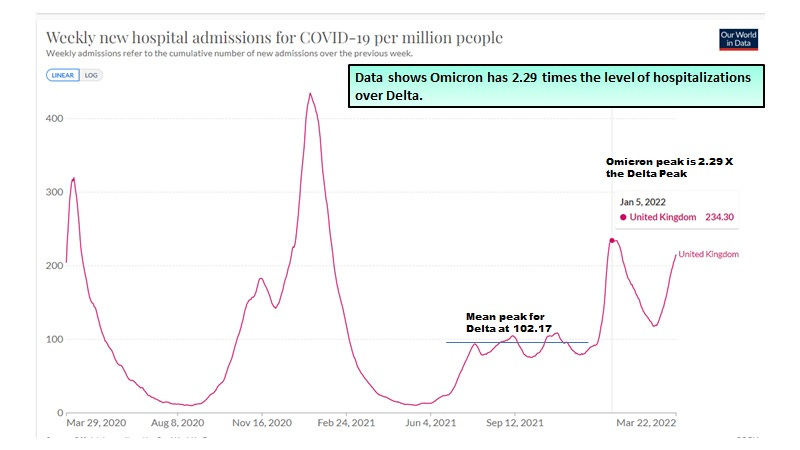
Image 3. Omicron indeed has higher peak levels of hospital admissions than Delta.
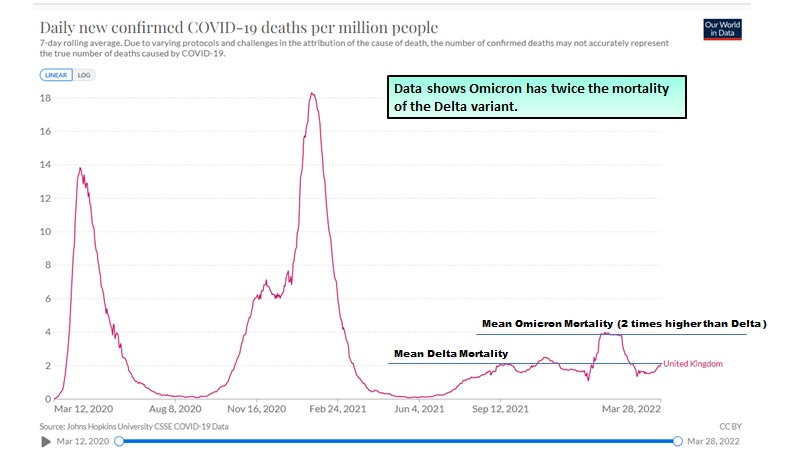
Image 4. Omicron also has higher peak levels of mortality than Delta.
For the Delta wave there were 295.67 deaths per million (June 4, 2021 - December 28, 2021) and for the Omicron wave there were 241.31 deaths per million (December 29, 2021 - March 27, 2022).
Along these lines of initial evidence for the beginnings of herd immunity, the Omicron variant infection despite significant mortality (compressed into a shorter duration) appears to be enhancing heterologous protection against all cause mortality consistent with the boosting of trained innate immunity (Image 5). This boosting is needed to provide sterilizing immunity to end the pandemic.
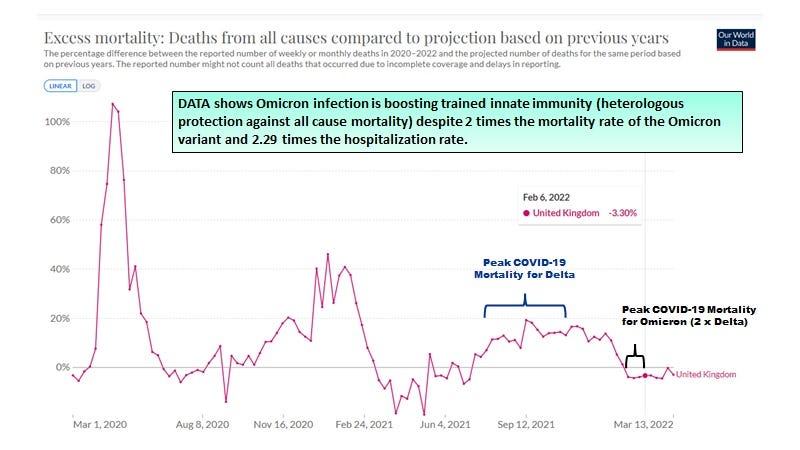
Image 5. Unlike the Delta (which was putatively selected for by the spike specific vaccines), Omicron (not selected by spike vaccines and which may have originated in the house mouse) appears to boost trained innate immunity (heterologous protection) as evidenced by negative excess all cause mortality.
If we look at recent data from the US, in Image 6, we see that for the Omicron variant there is a loss of VE against Omicron symptomatic infection at 3 months with the BNT162b2 vaccines when it cross the value of one (no difference of risk between 2 dose vaccinated and the unvaccinated after 3 months). On the right is shown that it takes 6 months to reach this for those who were vaccinated with the mRNA-1273 vaccine (which is twice the dose of BNT162b2).
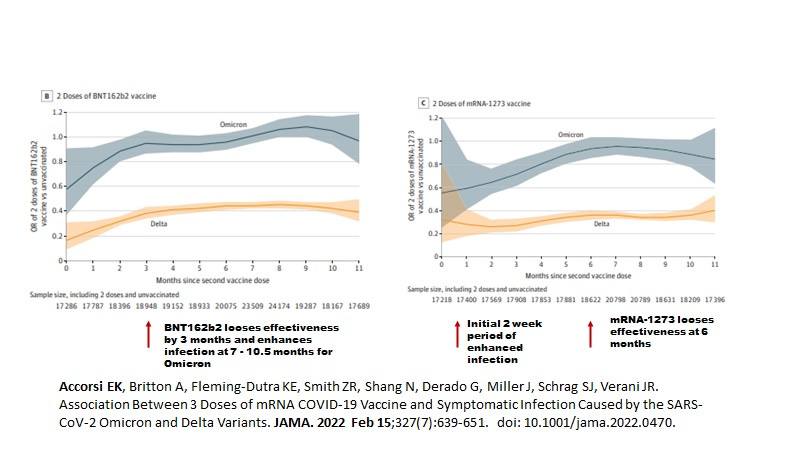
Image 6. Data from Accorsi EK et al. JAMA February, 2022 showing loss of VE against Omicron infection at 3 months (BNT162b2) or 6 months (mRNA-1273) after the 2nd dose (Dec 10, 2021 to Jan 1, 2022 in 49 States in the USA).
However, if we use the 50% VE rule and apply it to the OR (ie. cutoff at 0.5) we see that both vaccines fail to control omicron at all times after the second dose (Image 7).
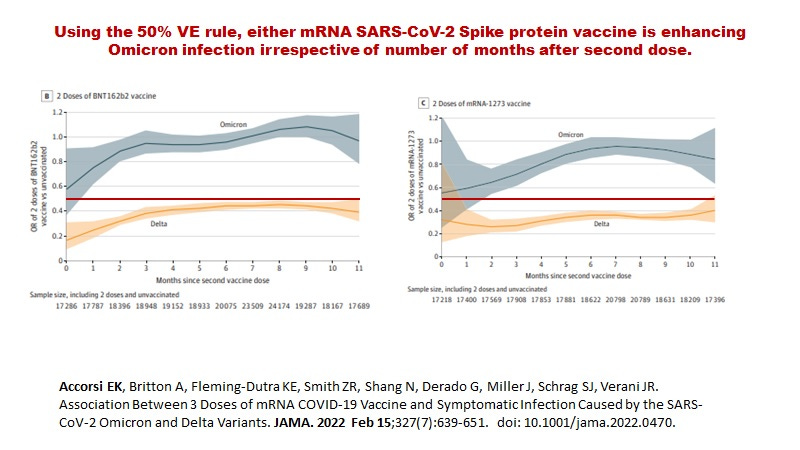
Image 7. The New 50% VE Rule applied to the data from Accorsi EK et al. JAMA February, 2022 showing loss of mRNA vaccine VE against infection across the board for the Omicron variant after the 2nd dose.
In a recent analysis of the Omicron versus the Delta wave in a Los Angeles hospital, Modes ME et al (MMWR February 11, 2022) reported that for the Delta variant the mortality rate was higher in the 2 dose vaccinated (10.6% ) when compared to the unvaccinated (7.9%). For the Omicron variant, the mortality rates were lower and more similar at 2.70% for the 2 dose vaccinated and 3.37% for the unvaccinated. Interestingly, the median ages for hospitalizations were significantly higher in the unvaccinated category for the Omicron (64 years of age) over the Delta wave (54 years of age) whereas for the fully vaccinated there was no difference (Omicron 69 years and Delta 71 years of age). Altogether these findings are consistent with the notion that vaccination may increase mortality against a vaccine selected variant, but may have little impact on Omicron. This substantiates the finding based on the 50% rule applied to the Accorsi et al (2022) data in Image 7 that little protection against Omicron is offered by vaccination to the spike protein wild type Wuhan strain.
In summary, there is likely an increase in absolute rates (per 100,000) for infections, and possibly hospitalizations and mortality associated with SARS-CoV-2 when the VE falls below 50% or the OR (odds ratio) increases above 0.50.
While public health leaders and governments are calling for more booster shots, we are reminded that boosting only serves to prolong the pandemic with higher rates of hospitalizations and deaths. It is time to abort the erroneous notion that boosting protects the population when in fact it just makes things worse. There is a urgent need to abort the development, testing and/or EUA approval of omicron specific vaccines, which will undoubtedly, restart a new pandemic. We need to petition the government against this looming catastrophe of omicron specific vaccines and booster shots of vaccines.
Instead we need to use ivermectin based protocols to treat symptomatic disease early to quell the morbidity and mortality of the pandemic and most importantly, to restore sterilizing immunity by trained innate immunity even in the most at risk.
Please have a look at the study by Dr. Bhakti et al on www.doctors4covidethics.org this week.
I am still working through the paper, page 33-34 is discussing ADE in the Pfizer/Moderna applications. Likely not acceptable for mainstream publication, it would be a good start for litigation.
They don't include your HERV-K102 chemistry. I will still watch for molecular explanations, theirs are generally at the macromolecule and tissue levels.