The COVID-19 Vaccines Should Have Been Taken off the Market by Early February 2021 Vaccine Safety Experts Say

Two outspoken experts on the safety of COVID-19 vaccines, Dr. Peter McCullough, M.D. (a cardiologist who specializes in COVID-19 preventative medicine and an expert in epidemiology and drug approval) and Dr. Marian Laderoute, Ph.D. Medical Sciences-Immunology (an immunologist with experience in the regulation of biological products and their post-market surveillance, and a global expert in immunosenescence and how the human body protects against novel pandemic RNA viruses) have declared that the emergency use authorization (EUA) for the COVID-19 vaccines should have been rescinded by early February 2021.
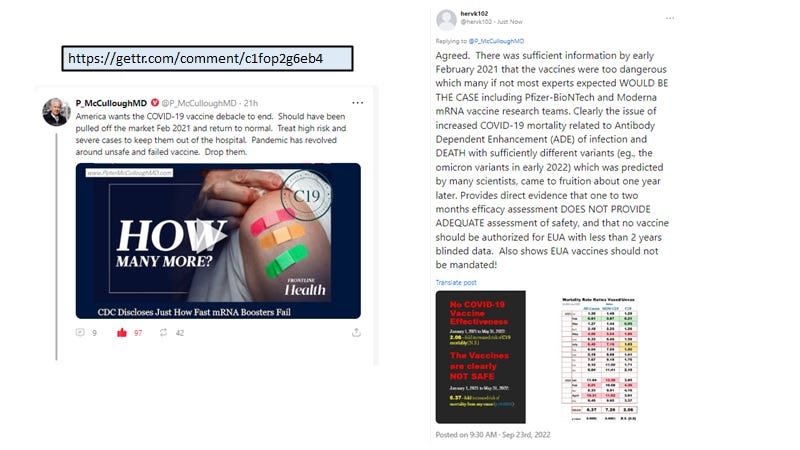
This stance is based on the findings compiled by Dr. Laderoute September 22, 2022 from the UK Office for National Statistics data released on July 6, 2022 that revealed all-cause mortality rates per 100,000 person years were significantly higher in the vaccinated over the unvaccinated (Image 1).
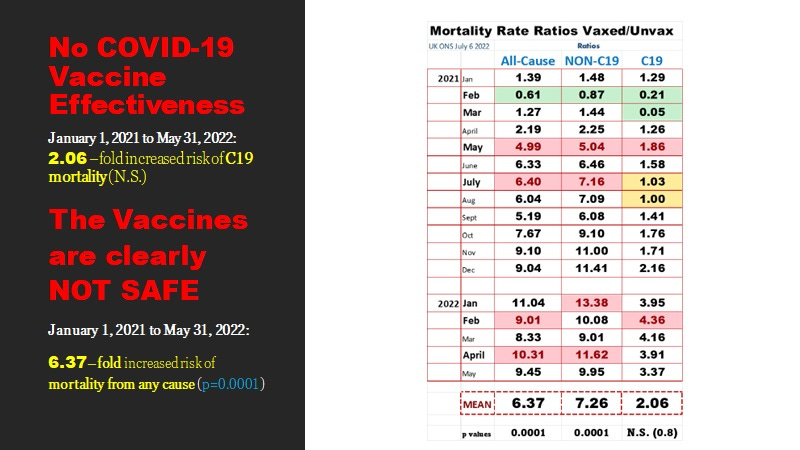
Image 1. Data Compiled from the UK Office for National Statistics (ONS) Released July 6, 2022 Clearly Indicates the COVID-19 mRNA Vaccines are NOT SAFE nor Effective.
https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/deaths/bulletins/deathsinvolvingcovid19byvaccinationstatusengland/deathsoccurringbetween1january2021and31may2022
The all-cause mortality ratio test is the definitive or gold standard used to establish that the benefits in preventing COVID-19 deaths by vaccination do not outweigh the risks of the vaccines causing more or equivalent number of deaths but by other causes. In other words, it would not make sense to approve an intervention which merely substitutes one cause of death for another. However, here we are detecting a 6-fold or higher all-cause mortality associated with vaccination with a very strong p value (indicator of high probability that the two rates are quite different and is unrelated to chance) as shown in Image 1.
Indeed, as more people got the second and then the third dose (October 2021), mortality rates escalated and were disproportionately higher with the ever vaccinated group over the unvaccinated. This demonstrated that the toxicity of the vaccines showed a dose response. This further strengthened the argument that the COVID-19 mRNA vaccines are inherently toxic and hazardous to human health.
Dr. Laderoute clarified that the ever vaccinated mortality rates reported by the ONS in their original tables in the report of July 6, 2022 appeared to be inappropriately adjusted downward, a problem noted previously for an earlier version of the same data by Jessica Rose and colleagues in December 2021 [1]. Instead, Dr. Laderoute added up all the mortality rates for each of the vaccination scenarios to derive the total for the ever vaccinated (ie., those who received at least one dose and up to 3 doses of COVID-19 vaccine) and then this was compared with the unvaccinated rates to derive the all-cause, non-COVID-19 (non-C19) and COVID-19 (C19) associated mortality rate RATIOs shown in Image 1. Thus, the ONS report failed to arrive at the same conclusion that the COVID-19 vaccines were not safe nor effective allegedly due to data tampering which underestimated the mortality rates for the ever vaccinated.
In Image 1, we can see that in January 2021 in the UK the ratios for the mortality rates of the vaccinated over the unvaccinated (Vaxed/Unvax) were all over 1.00 meaning there were more deaths per 100,000 person years for the ever vaccinated than the unvaccinated. These results would have been available in the UK (and in other countries around the world) at the end of January with analysis during the first week of February 2021. Why these data were not openly announced and made available for discussion around the first week of February 2021 through the public health agencies around the world including the WHO, will be the subject of future inquests on the failures of the global SARS-COV-2 pandemic responses by responsible parties and how this led to excessive deaths.
That the COVID-19 vaccines would not be safe and would in all likelihood not only lead to increased infection rates in the vaccinated but also higher COVID-19 mortality rates with time was expected based on the selection of SARS-CoV-2 immune escape variants by the antibodies produced to spike protein following the receipt of the second dose of COVID-19 vaccine [2]. Virtually all papers had shown that antibodies to spike protein correlated with progression to more severe COVID-19 disease and paradoxically, NOT with protection against severe disease [2].
Although somewhat complicated, through a process known as antibody dependent enhancement (ADE) the antibodies produced following the second dose of vaccination select for immune escape variants in the upper respiratory tract (URT). These selected variants then get transmitted to new hosts who if vaccinated have an increased risk of infection due to ADE [2]. As well ADE by causing the infection of macrophages/monocytes which are critical to the host defense against pandemic RNA viruses, diminishes the host’s ability to clear the virus. This potentially results not only in higher viral loads in the URT, but progression to more severe disease including death [2].
No selection of immune escape variants prior to the COVID-19 vaccine rollouts
Indeed various lines of evidence showed very little selection of immune escape variants occurred worldwide prior to the introduction of the mass COVID-19 vaccination campaigns. Why little or no selection of variants occurred during natural infection in the unvaccinated such as during the first year of the pandemic is explained elsewhere [2]. As Dr. Laderoute notes, it was the second dose of the mass vaccination campaigns which caused the selection of variants, which dropped vaccine effectiveness and this led to poorer outcomes [2].
Dr. Laderoute suggests that it is the virus non-specific protection offered by trained (innate) immunity involving the HERV-K102 protection system of lipid body negative (M1-like) proinflammatory foamy macrophages (Image 2) that provides protection against pandemic viruses like SARS-CoV-2 [2] .
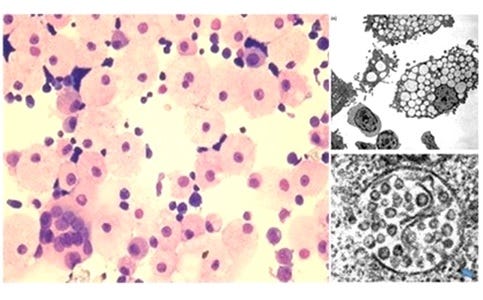
Image 2. The Lipid Body Negative, Pro-Inflammatory (M1-like) Foamy Macrophages (LB-FMs) Produce HERV-K102 Particles Which are then Released by Cell Lysis on Day 7 [3-5] and Provide Protection Against Severe COVID-19
However, these cells are targeted by SARS-CoV-2 in the URT (sebocytes of sebaceous glands) [6], in the LB-FMs in the lower respiratory tract [7], and systemically in the tissues where entry into the ACE2 negative cells is mediated by ADE. This is why the spike antibodies are so dangerous and correlate with progression and not protection against severe COVID-19.
Indeed, it can be argued that it is the trained (innate) immunity protection which wanes by 6 months after vaccination and not so much the antibodies specific to spike protein.
It is notable that most pseudovirus neutralization assays based on production of the pseudovirus in human cells rather than green monkey cells, inadvertently allows for the detection of innate neutralizing antibodies to HERV-K102 envelope. This is because human but not monkey cells transfected with vectors express HERV-K102 on the cell surface which then becomes incorporated into the ‘pseudoparticles’ allowing for these innate antibodies to neutralize the pseudoparticles. Moreover, these innate anti-HERV-K102 envelope antibodies appear to be abundant in persons infected with pandemic RNA viruses such as HIV-1 [5]. These innate antibodies to HERV-K102 envelope, the HERV-K102 protector particles in plasma [5] and innate T cells directly recognizing HERV-K102 envelope epitopes in the absence of MHC [reviewed in 4], may serve to clear the pandemic RNA virus without recognition of the spike or other virus-specific antigens.
The adaptive immunity response involving B cell responses specific to virus antigens is not appropriate for the individual nor at the population level during a a pandemic with an RNA virus.
This is because by the time the adaptive immunity engages at 7 to 10 days, the virus has already mutated so that the specificity of the spike antibodies is always going to be too late to be effective, and worse, more capable of ADE. At the population level, pre-existing antibodies to spike protein due to mass vaccination, will select for escape mutants in the upper respiratory track [2] which then become transmitted to others. We can see in the data in Image 1, that there was only one month, February 2021 where the vaccinal antibodies saved more lives from COVID-19 and including all-cause mortality before the selection of variants (by mass vaccination) abrogated the protection by vaccinal antibodies to the wild type Wuhan strain of spike. We know in an immunocompromised human host it takes only 10 days for the selection and dominance of an immune escape variant as selected by neutralizing monoclonal antibodies to spike protein [8].
So boosting may temporarily reinvigorate this innate immunity protective response, but at the same time 1) increases the levels of the dangerous spike specific antibodies and 2) exposes the host to toxic spike protein. The combination of these two effects may serve to annihilate the innate immunity protection which may take less and less time with each booster dose, due to induction of immunosenescence by spike protein binding to BSG on the ACE2 negative protector foamy macrophages (see Images 2 & 3).
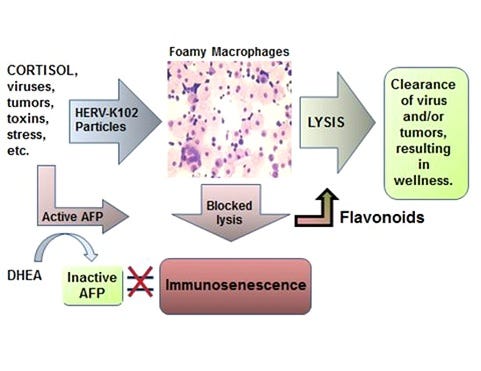
Image 3. The New Immunosenescence Paradigm [9,10] Defined as the Failed Lytic Release of Protector HERV-K102 Particles from Foamy Macrophages is Reversible by Alpha-fetoprotein (AFP) Antagonists such as Zinc, Flavonoids and Possibly Ivermectin [11]
Booster COVID-19 doses may trigger immunosenescence which not only immunosuppresses the host (making them much more vulnerable to tumors and infections of any type) but which also contributes to onset or progression of chronic illness such as cardiovascular diseases including hypertension, insulin resistance, diabetes, metabolic syndrome, autoimmunity, cancer and central nervous system diseases such as Alzheimer’s disease.
For example, spike protein on its own in the presence of antibodies to spike protein, would favor binding of spike protein to BSG on the LB-FMs in the same manner as Ren et al have described in the bronchoalveolar lavage fluid samples of severe COVID-19 patients [7]. This might result in the triggering of immunosenescence (Image 3) [9] and thereby increases the risks of chronic illness including cardiovascular disease [10], cancers, autoimmune conditions, diabetes, and so on. The induction of immunosenescence exacerbated by the deadly antibodies to spike protein might explain in part how these diseases are contributing to the high non-COVID-19 mortality reflected in Image 1.
Thus, the claims that COVID-19 boosted individuals appear to be immunosuppressed and at a higher risk of infections, as well as a higher risk of cancer, cardiovascular disease, and Alzheimer’s disease appear to be well-founded in the science of immunosenescence.
In summary, the data in Image 1 show that wishful thinking had no place in taming the SARS-CoV-2 pandemic, and that public health authorities and governments across the world dropped the ball first by rushing the EUAs and secondly by failing to determine, report and follow the science on the impact of the experimental vaccines on human mortality, critical during the first few weeks of the vaccine roll-out.
Boosters recommended by governments may be placing its citizens at much higher risks of non-COVID-19 (about 11-fold) than omicron associated deaths.
___________________________________________
REFERENCES
Neil M, Fenton N, Smalley J, Craig C, Guetzkow J, McLachlan S, Engler J, Russell D, Rose J. Official mortality data for England suggest systematic miscategorisation of vaccine status and uncertain effectiveness of COVID-19 vaccination. Research Gate December 2021. DOI: 10.13140/RG.2.2.14176.20483. https://www.researchgate.net/publication/356756711_Latest_statistics_on_England_mortality_data_suggest_systematic_mis-categorisation_of_vaccine_status_and_uncertain_effectiveness_of_Covid-19_vaccination.
Laderoute M. Trained immunity involving HERV-K102 activation may promote recovery from COVID-19 providing a new vaccination paradigm against pandemic RNA viruses. (81 pages, 188 references, submitted). See abstract below.
Laderoute MP, Larocque LJ, Giulivi A, Diaz-Mitoma F. Further evidence that human endogenous retrovirus K102 is a replication competent foamy virus that may antagonize HIV-1 replication. Open AIDS J. 2015 Dec 7;9:112-22. doi: 10.2174/1874613601509010112.
Laderoute MP. Clues to finding correlates of risk/protection for HIV-1 vaccines [version 2; peer review: 2 approved with reservations] F1000 Research 2018, 6:868. https://doi.org/10.12688/f1000research.11818.2.
Laderoute MP, Giulivi A, Larocque L, Bellfoy D, Hou Y, Wu HX, et al. The replicative activity of human endogenous retrovirus K102 (HERV-K102) with HIV viremia. AIDS. 2007 Nov 30;21(18):2417-24.
Ziegler CGK, Miao VN, Owings AH, Navia AW, Tang Y, Bromley JD, et al. Impaired local intrinsic immunity to SARS-CoV-2 infection in severe COVID-19. Cell. 2021 Sep 2;184(18):4713-4733.e22. doi: 10.1016/j.cell.2021.07.023.
Ren X, Wen W, Fan X, Hou W, Su B, Cai P, et al. COVID-19 immune features revealed by a large-scale single-cell transcriptome atlas. Cell. 2021 Apr 1;184(7):1895-1913.e19. doi: 10.1016/j.cell.2021.01.053.
Jensen B, Luebke N, Feldt T, Keitel V, Brandenburger T, Kindgen-Milles D, et al. Emergence of the E484K mutation in SARS-COV-2-infected immunocompromised patients treated with bamlanivimab in Germany. Lancet Reg Health Eur. 2021 Sep;8:100164. doi: 10.1016/j.lanepe.2021.100164.
Laderoute MP. A new paradigm about HERV-K102 particle production and blocked release to explain cortisol mediated immunosenescence and age-associated risk of chronic disease. Discov Med. 2015 Dec;20(112):379-91.
Laderoute M. The paradigm of immunosenescence in atherosclerosis-cardiovascular disease (ASCVD). Discov Med. 2020 Jan-Feb;29(156):41-51.
Laderoute M. Ivermectin may prevent and reverse immunosenescence by antagonizing alpha-fetoprotein and downmodulating PI3K/Akt/mTOR hyperactivity. Open Heart, April 29, 2021. https://openheart.bmj.com/content/8/1/e001655.responses#ivermectin-may-prevent-and-reverse-immunosenescence-by-antagonizing-alpha-fetoprotein-and-downmodulating-pi3k-akt-mtor-hyperactivity.