
Surprisingly...Plain & Simple
September 17, 2022

The Office for National Statistics in the UK provided informative data on July 6, 2022 which enables for the first time the ability to assess risk versus benefit of the COVID-19 vaccines (mostly the Pfizer-BioNTech mRNA vaccine was used in the UK), based on all-cause mortality.
https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/deaths/bulletins/deathsinvolvingcovid19byvaccinationstatusengland/deathsoccurringbetween1january2021and31may2022
The risk versus benefit analysis is required for approval of drugs, biological drugs and vaccines and is the most important test for determining safety and effectiveness.
All-cause mortality is needed for the assessment of interventions intended to reduce deaths such as the COVID-19 vaccines.
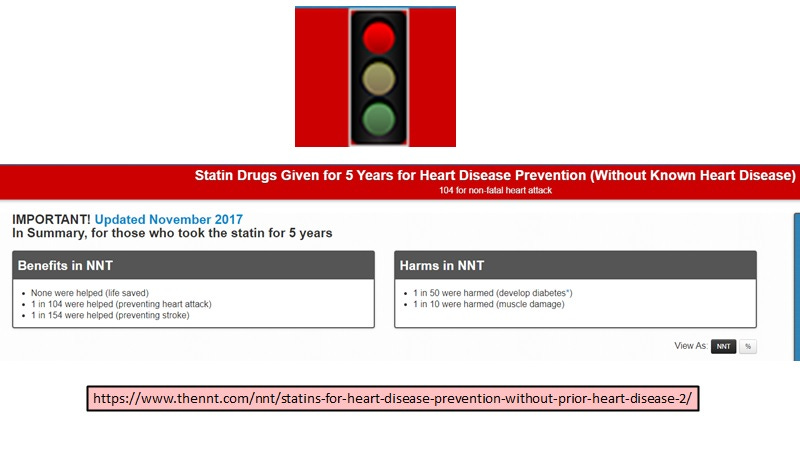
Not all drugs/interventions reduce deaths and for these one would instead calculate the ‘number needed to treat’ (NNT) and compare this with ‘number needed to harm’ (NNH) [see https://www.thennt.com]. Many approved and commonly used drugs surprisingly are not recommended (get a red light) due to poor risk versus benefit ratios, shown here for statin use (5 years) in those without heart disease.
It should be noted that this critical test involving all-cause mortality was globally overlooked for the initial emergency use authorization (EUA) of the COVID-19 vaccines in December 2020 for adults as this data was not yet available.
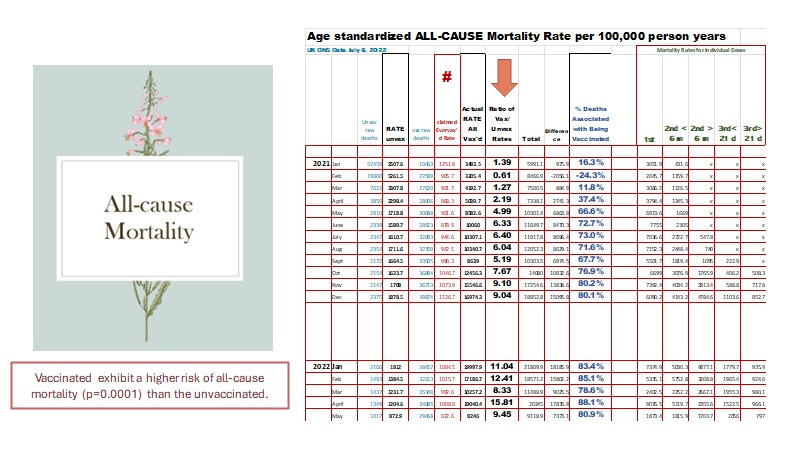
However, these informative AND CRITICAL data would have been available for the evaluation of subsequent EUA applications (info available after the very first month, January 2021 see below where the all-cause mortality rate ratio (per 100,000 person-years) was 1.39, the non-COVID-19 mortality ratio was 1.48 and the COVID-19 mortality ratio was 1.29 for deaths for the ever vaccinated over the unvaccinated).
In other words, the use of COVID-19 vaccines for younger and younger children, for booster shots, and more recently for the omicron hybrid booster shot (which was FDA approved on August 31, 2022 and CDC recommended on September 1, 2022) WOULD NEVER HAVE BEEN APPROVED AND THE INITIAL EUAs would have been RESCINDED.
The FDA, the CDC and their advisory groups did not request this data for US citizens nor considered this critical data published in earlier versions by the ONS (UK) for any of the subsequent EUAs.
The UK ONS data as shown in the next slide summarized by month shows there was only one month (February 2021) where the all-cause mortality for the mortality rates (per 100,000 person-years) of the ever vaccinated over the unvaccinated was less than one.
IN FACT, on average, for the 17 months of data covered by the ONS July 6 2022 report, the COVID-19 ever vaccinated over the unvaccinated were at a 6.90-fold increased risk of death from any cause (all-cause mortality) with a p value of 0.0001 meaning the results are statistically very highly significant.
Therefore, there is no doubt that the COVID-19 vaccines are THEMSELVES associated with an increased risk of death and thus, SHOULD BE IMMEDIATELY REMOVED FROM THE MARKET.
Fun FACTS:
In addition to showing all-cause death rates (per 100,000 person-years) were higher in the vaccinated over the unvaccinated, the C19 mortality ratios confirmed the expected existence of Antibody Dependent Enhancement (ADE) of infection contributing to death. This was evident since May 2021 (ratio of 1.86) coincident with the emergence of the delta variant (caused by selection due to vaccination generation of spike antibodies).*
Note that the earlier mortality ratio in January 2021 of 1.29 was likely due to higher transmission of SARS-CoV-2 at the time and place of first dose vaccination whereas these large gatherings of highly susceptible people did not occur in the unvaccinated.
Note also, since the omicron variant emerged late in December the risk of COVID-19 mortality was about 4-fold higher in the vaccinated over the unvaccinated while non-COVID-19 mortality ratios were elevated 10-fold. In other words, the neutralizing antibodies generated against the Wuhan variant, are more likely to cause harm presumably through ADE, the more distantly related the variant’s spike protein is to the wild type Wuhan variant. Sudden increases in risk then may correlate with emergence/dominance of a new immune escape variant. The increased COVID-19 mortality risk of vaccinated over unvaccinated with time is consistent with increased virulence. Paradoxically omicron does not induce the same level of pneumonia as the delta variant, but it seems to be more deadly presumably related to the higher number of persons infected and possibly the toxic effects of spike protein.

It is not precisely known how the vaccine contributes to death in the absence of SARS-CoV-2. A recent paper on 4 deaths (3 sudden deaths at 1, 2, and 3 days and 1 at 10 days post vaccination) involving cytokine storm [Murata K et al., Frontiers in Immunology, 15 August 2022] indicates the KEGG pathways upregulated in blood involved neutrophil degranulation, upregulated cytokine signaling, glycolysis, NFKB1 signaling, FC gamma mediated phagocytosis, myeloid cell activation, and tuberculosis when compared to accidental or homicidal deaths of those who had been vaccinated. Moreover, 6 differentially expressed upregulated genes were FCGR2A (commonly implicated in ADE), S100A8, OLR1, CXCL8, CEBPB, and IGFBP2 which further implied the M1-like lipid body negative, pro-inflammatory foamy macrophages (LB-FMs) in the dysfunction which led to sudden death. Table 9 from the July 6 2022 ONS report shows while most non-COVID-19 deaths occurred at 12 weeks or later, a significant number occurred at 1 week which doubled by 4 weeks. The latter would be consistent with the notion that the enhancement of spike specific antibodies which occurs after 7 days may exacerbate the risk of sudden death. In theory once the spike specific antibodies are made, this would increase the likelihood of the spike protein from the administered vaccine binding and thus triggering the BSG positive but ACE2 negative LB-FMs as reported for the lower respiratory tract SARS-CoV-2 infections by Ren X et al [Cell, 2021]. It is known that both uninfected and infected macrophages contribute to cytokine storm in patients with severe COVID-19 [Laderoute, submitted]. Therefore it is possible that the spike protein by binding to BSG on the LB-FMs causes their dysfunction leading to cytokine storm. This hypothesis would be easy to test such as in the humanized mice discussed by Kenney et al, 2022 [ Kenney DJ, O'Connell AK, Turcinovic J, Montanaro P, Hekman RM, Tamura T, et al. Humanized mice reveal a macrophage-enriched gene signature defining human lung tissue protection during SARS-CoV-2 infection. Cell Rep. 2022 Apr 19;39(3):110714. doi: 10.1016/j.celrep.2022.110714].
_________________________________
*Globally, there was essentially no significant evidence of selection of immune escape variants before the vaccines were introduced (See Our World in Data, COVID-19). In the UK, over 600,000 residents participated in vaccine clinical trials before December 2020, which would account for why the alpha variant emerged before mass vaccination in the UK. Also it has been argued that selection of the alpha and/or delta variants was not likely to occur under natural conditions, but would require the pre-existing antibodies to spike protein (ie., the vaccinal antibodies) to select for variants and to mediate their transmission from the upper respiratory tract in the first 5 days after SARS-CoV-2 infection [Laderoute M. Trained immunity involving HERV-K102 activation may promote recovery from COVID-19 providing a new vaccination paradigm against pandemic RNA viruses. submitted]. Also in Canada the emergence or dominance of the alpha then delta variants were linked to the administration of the second dose of COVID-19 vaccines or with the loss of trained innate immunity from the first dose [see article below and Laderoute, submitted].

As best as I can tell from the Pfizer-BioNTech 6 month report [Thomas SJ, Moreira ED Jr, Kitchin N, Absalon J, Gurtman A, Lockhart S, Perez JL et al; C4591001 Clinical Trial Group. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine through 6 Months. N Engl J Med. 2021 Nov 4;385(19):1761-1773. doi: 10.1056/NEJMoa2110345] all the deaths that occurred within the first 7 days that were SARS-CoV-2 positive or not after the administration of the first and/or second doses of vaccine (BNT162b2 or placebo) were EXCLUDED FROM THE PRESENTED DATA IN THIS PAPER. However the VAERS data (see slide 5 of the above slide deck) shows the vast majority of VACCINE deaths occurs within the first 7 days, and more commonly within 2 days. Thus, Pfizer-BioNTech appears to have willfully hidden crucial data on vaccine safety aided and abetted by NEJM. This may constitute fraud which invalidates the exemption against liability of the vaccines.
If it is anything we have learned from the vaccine fiasco, it is that democratic societies need laws: 1) forbidding the mandating of medical interventions such as vaccines including during emergencies or as a requirement for attending schools ; 2) forbidding the FDA, CDC, NIH, WHO, hospitals and any other government agency from dictating what medical interventions are legally acceptable or what prescribed drugs can or cannot be used off-label; 3) blocking the ability of vaccine manufacturers and others to request or obtain exceptions from liability for themselves or anyone else involved in the procurement, administration or recommendations of vaccines whether emergency access or not; 4) forbidding the exemption of vaccine manufacturers from liability; 5) stop the advertising of medical products on any media (TV, social media, billboards, etc) as allowed in the USA which has led to captured agencies and media; 6) forbidding the FDA and other regulatory agencies around the world from accepting money or fees for the review of products where instead the taxpayers would pay the costs; and 7) prohibit hospital incentives for diagnostic tests, treatments or deaths but to provide incentives for the reporting of adverse events and deaths.