

Natural Immunity is Similar Albeit Better than the Third Dose (Tolerizing) COVID-19 Vaccine for All-Cause Mortality in the Aged
Natural Immunity is Similar Albeit Better than the Third Dose (Tolerizing) COVID-19 Vaccine for All-Cause Mortality in the Aged
All-Cause Mortality is KEY



Steve Kirsch has repeatedly emphasized the dangers of COVID-19 vaccines saying natural immunity is much better when it comes to all-cause mortality.
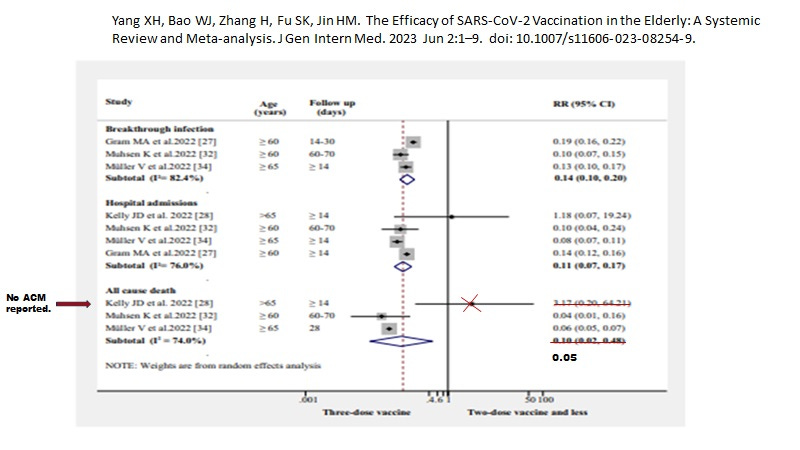
The above data imply that those at highest risk of COVID-19 mortality; namely the 65+ are much better off with no vaccinations than going through 3 doses to get rid of the antibody dependent enhancement (ADE) problem of infection of macrophages related to spike IgG1 and IgG3. (Recall that the 3rd dose converts the dangerous IgG1 and IgG3 to the safer IgG4 which does not mediated ADE). Also, the more vaccines the higher the risk of infection (the Cleveland Clinic data and the UK data), meaning vaccination increases the duration of the pandemic.
Note that the first dose does provide significant all-cause mortality protection (like the UK data below see February 2021) consistent with “trained innate immunity” and heterologous protection (not only against infectious diseases and cancers but also all chronic diseases).
While the Yang et al data (above) indicate the 4th dose may improve all-cause mortality over the 3rd dose in the 60 + population, this benefit may only be short term (30 days or even 60 days), as the UK ONS data (below) indicate all-cause mortality remains well above the unvaccinated over the entire period covered.
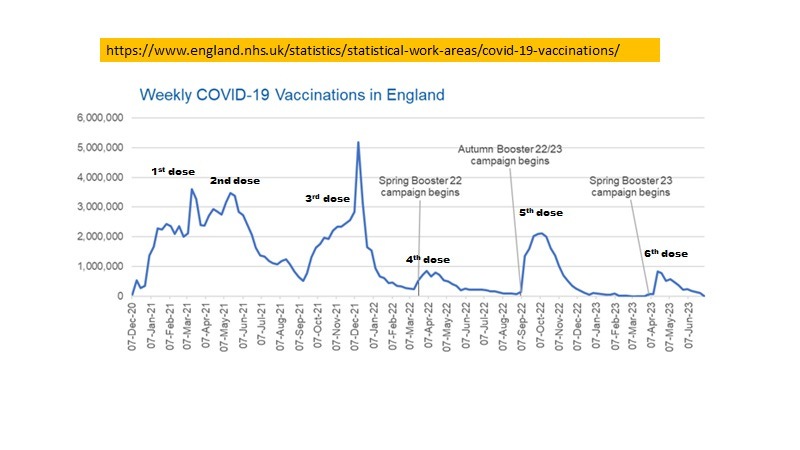
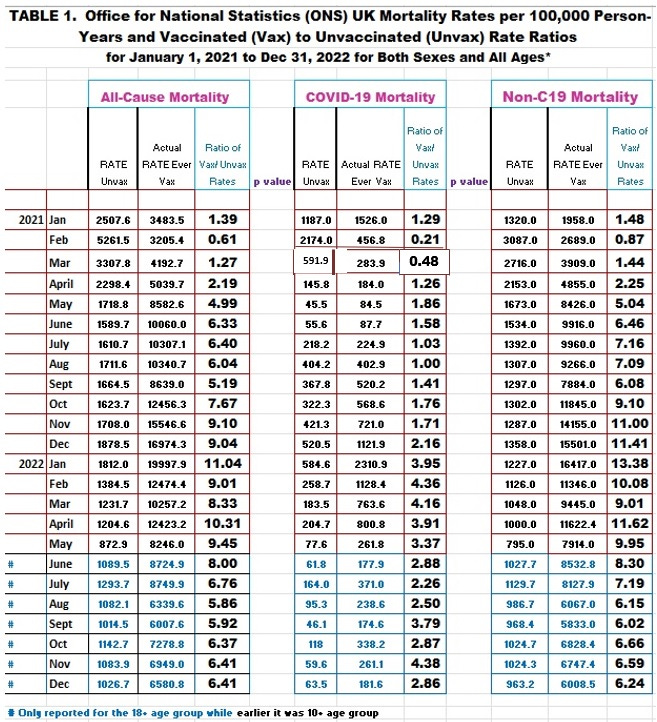
The only time that All-cause mortality was acceptable was in February 2021 in the UK where about 96% of the immunized population had only one dose (trained innate immunity). Note that the increased all-cause mortality due to vaccination persists longer term. When does it end? No one knows.
I prefer the functional term "injected" to the fluid definition "vaccinated."
Definitions ave varied to conceal the M&M of the first two weeks, and some of the English reports have extended the term "vaccinated" to only include the subjects reported 21 days post-injection.
Were the first two days' mortality after injection counted? This is certainly not clear from the table you have presented from the UK ONS. I have not yet reviewed the original data set, but I don't recall a similar conclusion from Joel Smalley's <metatron.substack.com> analysis.
This (intentional) confusion of definitions has pervaded the entire Covid narrative making assessment of almost anything difficult or impossible.
I first read about ADE in a CMAJ article in Nov., 2022, and had to review the definitions and mechanisms a few times to understand the pathophysiology and outcomes. Do we see the same pattern in the Cleveland Clinic study?
As the C19 diagnosis was so corrupt (PCR Ct 40 and above) it is difficult to accept any of these early statistics. Recall that most of the SARS-CoV-2 papers in 2020 and 2021 started with the assertion that C19 was 1.5% fatal. I have not seen retractions or corrigenda on any of these studies.
We must be continually vigilant in believing any analysis based on government statistics.
Thank You, Dr. Laderoute.
At 65 years of age I have been keeping my all-cause-mortality down as much as I can.
I am pleased to still be on the right track.
:-)