


Is the Conversion of IgG1/3 to IgG4 a GOOD or BAD Thing?
Does adaptive immune tolerance induced by the 3rd dose increase or decrease all-cause mortality?


A recent paper remarked on how repeated COVID-19 vaccination such as dose 3 of the mRNA vaccines generates the conversion of spike specific IgG1 and IgG3 antibodies to IgG4 (which are then devoid of inflammatory activity), and proposed that this immune tolerance to the SARS-CoV-2 spike protein could lead to increased all-cause mortality [Uversky VN et al., Vaccines, May 17, 2023].
Although they proposed this transformation of the isotype of spike antibodies from inflammatory to non-inflammatory by the third and subsequent doses might encourage chronic diseases, the actual mechanism seemed vague.
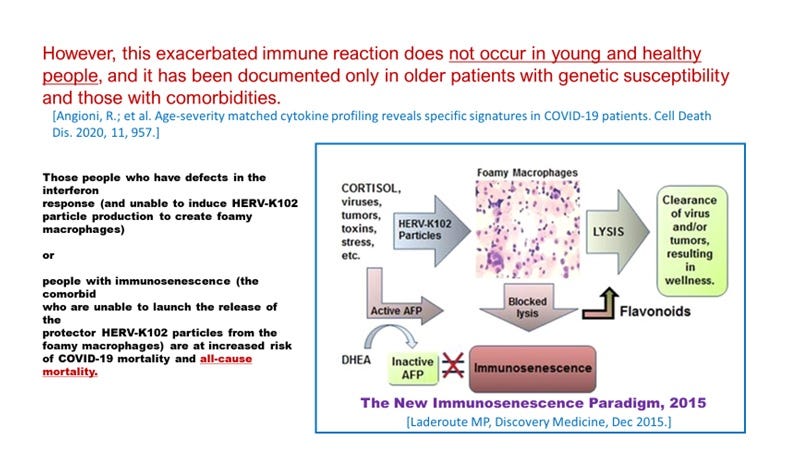
However, they provided a hint that these associated problems did not occur in the young or healthy and instead related to being older with co-morbidities, which implied that immunosenescence [Laderoute MP, Discovery Medicine, 2015] likely is at the heart of the issue.
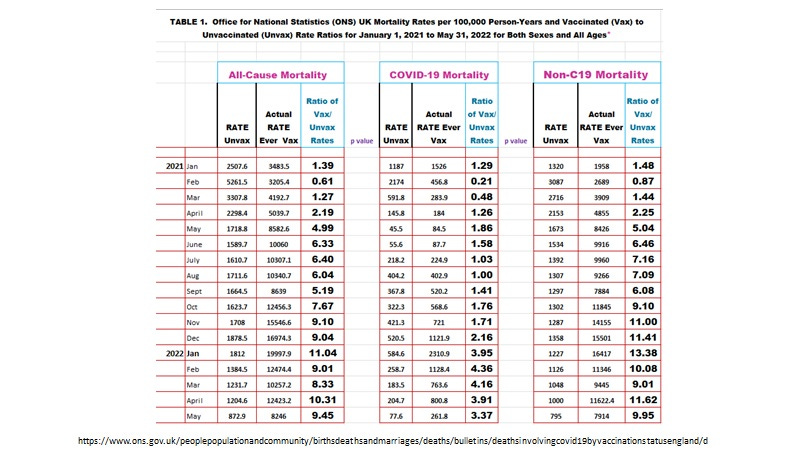
Before we get to the data on this issue at hand, we must understand that across all age groups the COVID-19 vaccines were extremely dangerous as shown in the data from the UK Office for National Statistics (ONS) for COVID-19, non-COVID-19 and all-cause mortality comparing unvaccinated to ever-vaccinated (rate per 100,000 person-years). This is very real for the non-COVID-19 mortality associated with the extreme toxicity of the mRNA gene therapies which masqueraded as vaccines.
The UK mortality data (reflecting the fact that the Pfizer-BioNTech COVID-19 mRNA vaccine was the most commonly used in the UK) stratified by number of doses for January 2022 to May 2022 obtained from The Expose [https://expose-news.com/2022/08/09/mortality-rates-lowest-among-unvacinated/], illustrates how three doses of mRNA vaccine,
abrogated the excess mortality associated with one or two doses completely in those unlikely to exhibit immunosenescence (age less than 60),
and partially in those 60 plus since some were at increased risk of immunosenescence. (The only exception to this narrative seems to be in the 70 to 79 year olds for May 2022 where the third dose led to increased mortality even over two and one doses.)
Note that the scale is log to the base 10 meaning the differences seem small but are in fact 10 fold higher. The unexpected more inhibition of the adverse effects of vaccination within the 90 plus group following the third dose could be due to higher death rates earlier in the pandemic leaving less 90 year-olds at risk due to immunosenescence.
In other words, only IgG1 and IgG3 can mediate antibody dependent enhancement (ADE) of SARS-CoV-2 infection into the macrophages but not IgG4. Thus, by conversion of the spike specific IgG into IgG4 stops ADE and returns the capability of the host to clear and inactivate SARS-CoV-2 via the trained innate immunity involving HERV-K102 particle production and release from the foamy macrophages.
However, the exception is that older people with immunosenescence who are vaccinated with 3 or more doses may still be at higher risk of all-cause mortality than the unvaccinated. (Is this because people in the unvaccinated category had lower prevalence of immunosenescence than those who received 3 doses???)
In summary, the association of IgG4 spike antibodies with increased risk of chronic diseases and death in older people with co-morbidities, is a misnomer, kind of analogous to whether the glass is half empty or half full. In fact, the IgG4 conversion of the spike antibodies abolishes the phenomenon of ADE, reducing the risks induced by one or two vaccine doses. Now the host only has to contend with immunosenescence blocking recovery in those with co-morbidities. Here, vitamins D and C along with ivermectin, zinc and flavonoids, would reduce the risks of immunosenescence on increasing all-cause mortality, whether the host is vaccinated or not.
In conclusion, the UK mortality data does not support the notion that the conversion of spike-specific IgG1/3 to IgG4 suppresses natural antiviral responses but instead enhances trained (innate) immunity involving HERV-K102 particle production in foamy macrophages by abrogating ADE. On the other hand it is true that the third doses of COVID-19 mRNA vaccines, place the susceptible host (older with comorbidities, ie., those with immunosenescence) at higher risk of all-cause mortality over the unvaccinated BUT at reduced levels when compared with one or two doses.
Generally, the third dose induction of IgG4 is a good thing, but it is far better to have avoided COVID-19 vaccination all together due to the extreme toxicity of the mRNA SARS-CoV-2 spike vaccines [Seneff S, Nigh G, Kyriakopoulos AM, McCullough PA. Innate immune suppression by SARS-CoV-2 mRNA vaccinations: The role of G-quadruplexes, exosomes, and MicroRNAs. Food Chem Toxicol. 2022 Jun;164:113008. doi: 10.1016/j.fct.2022.113008].
There might be a caveat with the second part of the conclusion. People who were not vaccinated (60 plus) or who only had two shots may have been those less likely to exhibit immunosenescence than those who did follow the vaccination to 3 shots. If this is the case, one might argue that the increased all-cause mortality risk due to 3rd shot vaccination merely pertains to levels of immunosenescence being higher in the 3rd shot vaccinated when compared with the unvaccinated. In other words the 3rd shot does not per se increase risk but reduces ADE risks.
The main reasons for the general lack of selection of immune escape variants prior to the vaccine roll-out in late December 2020 was because during natural infection, for the most part the innate immune system was able to clear or inactivate replication competent SARS-CoV-2 from the URT before the onset of the spike anti-IgG [Wolfel R et al., Nature, May 2020]. Perhaps more importantly, a growing body of evidence implies for natural infection unless the case of COVID-19 was severe/critical, there were few IgG1 or IgG3 antibodies to spike RBD in the nasal secretions and none in the saliva [Guerrieri M et al., Vaccines Basel, Dec 2021; Aksyuk AA Et al, Cell Rep Med Dec 2022]. However, with the second dose of COVID-19 vaccines (mRNA or virus vectored), these dangerous IgG antibodies to spike protein were commonly detected at high levels in the URT. It seems then the conversion only occurs systemically and not the URT since the omicron variants are much more transmissible???