


Imprinting versus ADE in terms of COVID-19 Vaccine Negative Effectiveness
The increased risk of COVID-19 and Non-COVID-19 mortality in the vaccinated over the unvaccinated persists with Omicron variants. Why?

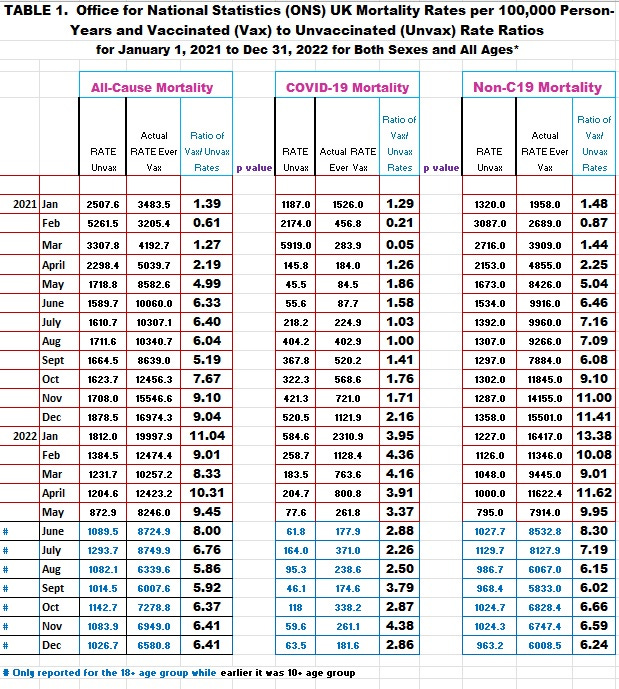
Image 1. The increased risk of mortality in the ever vaccinated over never vaccinated persists even with omicron which has dominated since the end of January 2022.
As well pointed out by Dr. Robert Malone, there may be many reasons why the COVID-19 vaccines show negative effectiveness.
It is also possible for one or more of the above to apply.
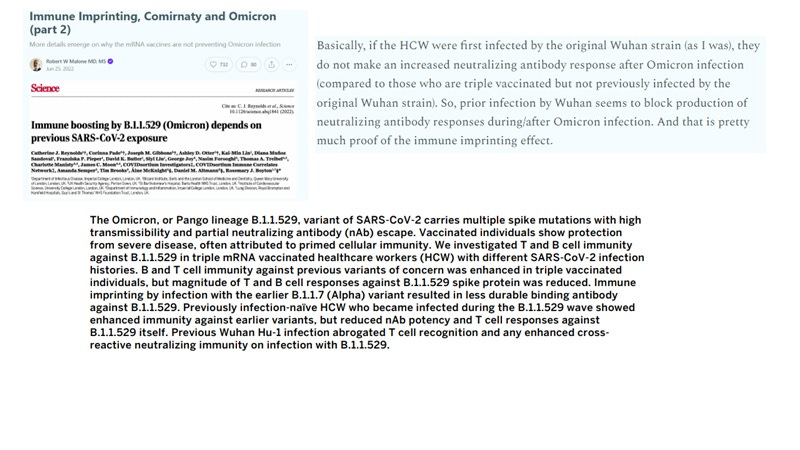
However, the argument is if a person had an infection with Wuhan, then vaccinated 3 times then infected with Omicron, the neutralizing antibody responses are blocked.
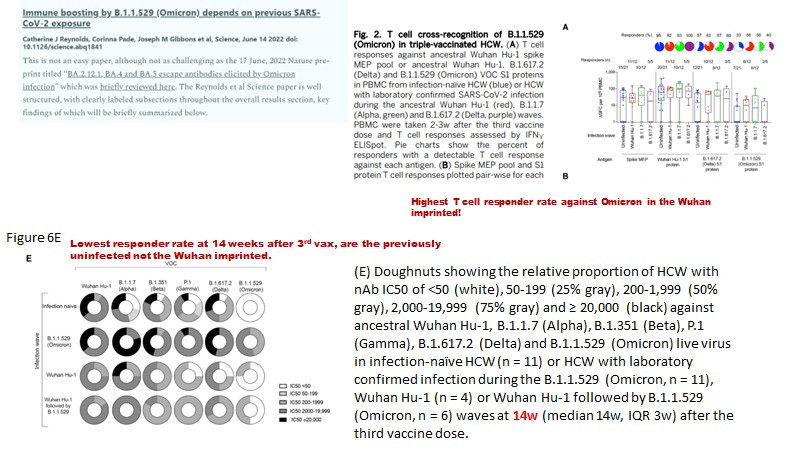
Image 2. Data from imprinting paper by Reynolds CJ et al, 2022 shows for T cells, that the highest responder rate against Omicron is in the Wuhan imprinted; and lowest NAb responder rate against Omicron was in the infection naive.
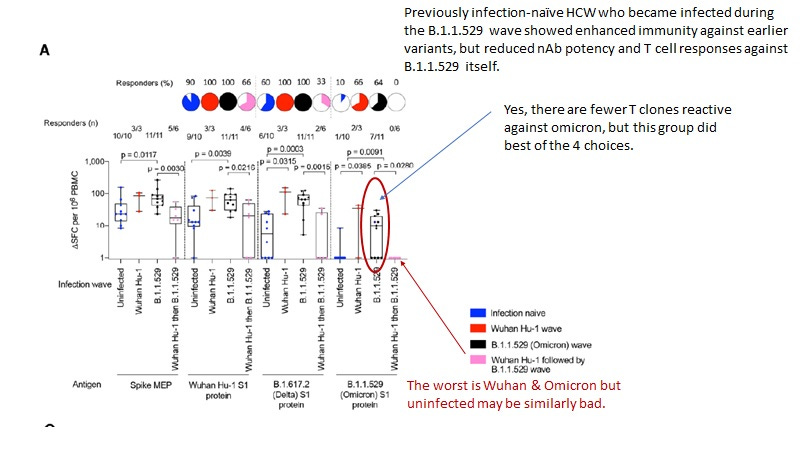
Image 3. For the T cell responder clones, the data are not that convincing (ie., remove 1/10 from uninfected would yield the same results from the Wuhan then Omicron infected).
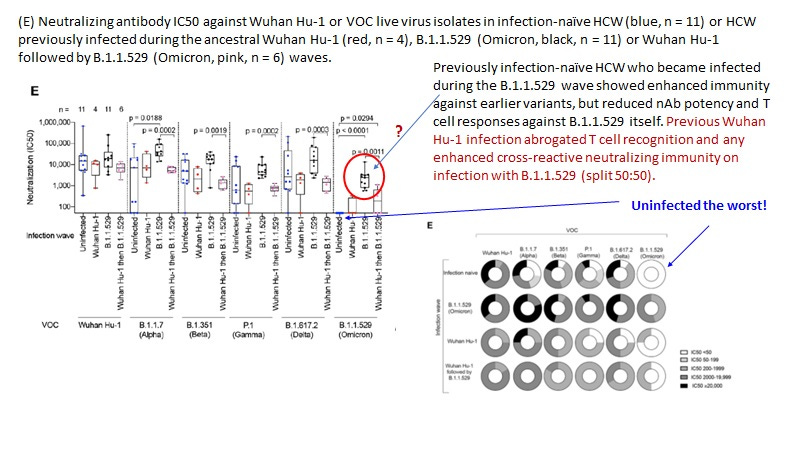
Image 4. Uninfected have the worst NAb levels, not the imprinted.
A key issue confronting the topic is what exactly is the correlate of protection against SARS-CoV-2? Is it adaptive IgG antibodies and/or neutralizing antibodies (NAbs) to spike protein?
The data in Image 1 shows the only time protection against COVID-19 and non-C19 mortality was detected in the UK associated with vaccination was in Feb 2021 when the vast majority of the people vaccinated (95.8 %) had not yet received the second dose (Image 5). Only the second dose is associated with spike IgG antibodies [Walsh EE et al, NEJM 2020; Chu L et al, Vaccine 2021].
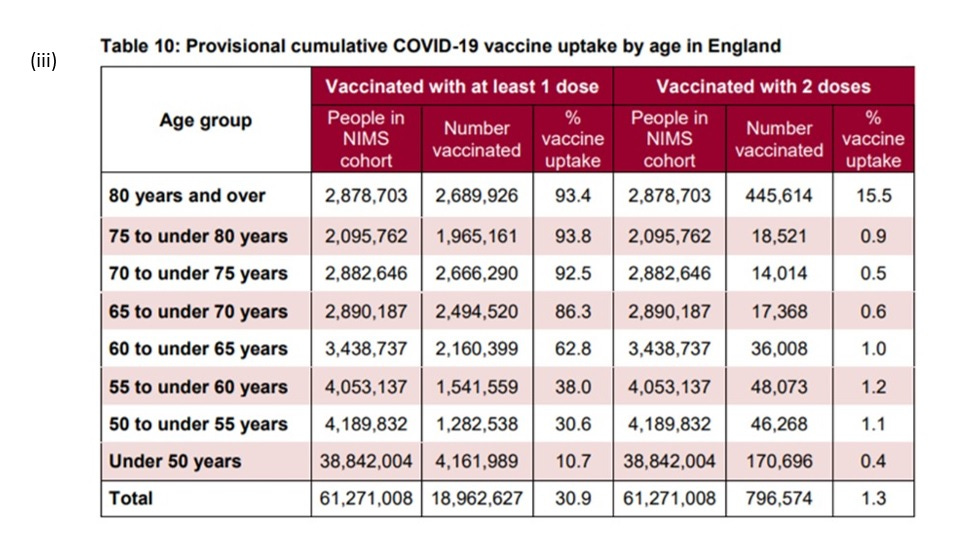
Image 5. By March 7 2021, only 4.2 % of the vaccinated in the UK had received the second dose. Therefore it is clear the antibodies to spike protein are not protective and cannot explain the protective response due to vaccination for Feb 2021.
https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/968513/Weekly_Flu_and_COVID-19_report_w10.pdf. Page 73/81; Table 10. Cumulative data up to week 9, 2021 for week ending March 7.
Thus, one can say a correlate of protection in part may relate to the absence of IgG to spike protein (reminiscent of the HIV-1 exposed seronegative cohorts that are resistant to HIV-1 acquisition).
Here is an abstract from a recently submitted review paper that talks about correlates of protection for COVID-19:
To date only the interferon response and vitamin D sufficiency which are attributes of innate immunity have been established as correlates of immune protection against SARS-CoV-2. Human endogenous retrovirus K102 (HERV-K102) is a non-pathogenic, replication-competent, foamy retrovirus unique to humans encoded at 1q22 of the human genome and herein has been identified as a salient component of trained (innate) immunity produced in macrophages. Accumulating evidence suggests during natural infection with SARS-CoV-2, it is not only the level but the advanced onset of the development of IgG antibodies to spike protein that are associated with progression to severe COVID-19. The name of the game is that the innate immune system must clear or neutralize live SARS-CoV-2 virions before the onset of the spike specific IgG. If not, neutralizing antibodies (NAbs) to spike protein select for variants and these variants enter macrophages by IgG antibodies to spike protein through antibody dependent enhancement (ADE) of infection. The SARS-CoV-2 infection of the WDR74 positive, lipid body negative foamy macrophages (LB-FMs) aborts the production and lytic release of the protector (HERV-K102) particles. This results in a loss of critical trained (innate) immunity needed to neutralize and clear pathogens. It also results in the loss of the cGAS-STING alternative amplification of interferon responses (spread by the released HERV-K102 particles that contain double stranded cDNA genomes). Moreover, the ADE mediated entry of SARS-CoV-2 into the LB-FMs also causes immunosenescence of the foamy macrophages which initiates and/or exacerbates chronic disease such as hypertension and heart disease, and results in the loss of immunosurveillance against infectious agents and cancer more generally. Finally, by SARS-CoV-2 conversion of the LB-FMs to LB+FMs which is prevented by sufficient vitamin D3 levels, this transition creates an immunologically-priviledged site for the replication and cell surface budding of the newly selected SARS-CoV-2 variants. In the upper respiratory tract (URT) these selected and replicating immune escape SARS-CoV-2 variants are then transmitted to others which prolongs the pandemic. In this paper how the novel and truly remarkable ‘virus anti-virus’ HERV-K102 protector trained (innate) immunity system may protect against pandemic viruses is explored. Data validating HERV-K102 activity and/or trained (innate) immunity with protection against pandemic RNA viruses and IgG spike antibodies with deleterious outcomes are presented including phylogenetic evidence and UK mortality data. Moving forward, vaccines able to safely trigger and boost HERV-K102 activation along with purified or cloned HERV-K102 particles and monoclonal antibodies to certain HERV-K102 envelope epitopes may provide new and useful active and passive immunization tools respectively, for pandemic preparedness that importantly, do not select for variants in the host or the population.
Incontrovertible evidence had emerged before the COVID-19 vaccines were authorized for emergency use that demonstrated IgG antibodies to spike protein were not protective but instead mediated progression to more severe COVID-19 disease including death [1-14].
Indeed, during natural infection with SARS-CoV-2, it was the more rapid and enhanced development of IgG antibodies to spike protein in higher risk older individuals [15-20] which was associated with progression to severe COVID-19 and not protection.
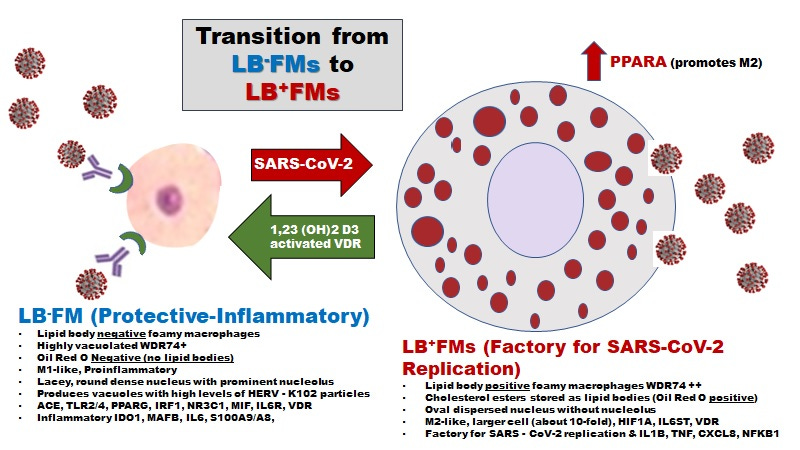
Image 6. Via Classical ADE in the Upper Respiratory Tract (URT, see Ziegler et al, 2021 [21]) involving FCGR2A on activated sebocytes (specialized lipid body negative foamy macrophages that constitutively produce the protector HERV-K102 particles) even with omicron there is selection of immune escape variants which then reproduce and become transmitted to others from the URT.
Generally there isn’t any IgG to spike protein in the URT unless the person is vaccinated [22]. Vaccination then contributes to selection of immune escape variants which did not generally happen prior to introduction of mass vaccination.
NOTES on Omicron
There are two types of ADE in vivo: the classical FCGR2A mediated ADE in the sebocytes in the URT [21] and the NOVEL switch of spike:ACE2 to Spike:BSG in the lower respiratory tract (LRT) [23].
Since omicron may have been derived from a house mouse, the interaction of omicron spike with human BSG potentially may not be sufficient to mediate infection of human myeloid cells, consistent with its reduced damage to the lungs and/or reduced replication in the periphery. Therefore, ADE would primarily relate to selection of omicron variants in the URT and transmission to others which perpetuates the pandemic. However, replication in the URT could release spike protein (made worse by the repeated exposure to COVID-19 vaccine) which apparently may activate the lipid body negative foamy macrophages that produce the HERV-K102 particles but also may cause immunosenescence of the macrophages related to apoptosis resistance and failure to release the protector HERV-K102 particles [24]. It may be the induction of immunosenescence by spike protein which drives the non-COVID-19 and COVID-19 associated excess mortality in the vaccinated over the non-vaccinated.
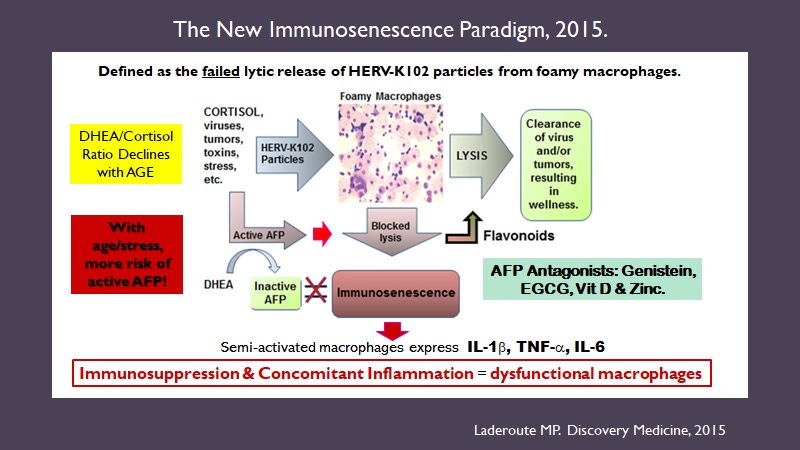
Image 7. The new immunosenescence paradigm, 2015 [25]. Dysfunctional macrophages cannot provide immunosurveillance against pathogens and tumors placing the host at higher risks. Also the production of proinflammatory factors initiates and causes the progression of chronic diseases such as cardiovascular, hypertension, metabolic syndrome, type 2 diabetes, AD, etc.
Based on work reported by Jensen et al, [26], it does not appear that the immunocompromised that remain SARS-CoV-2 positive actually select for variants as immune escape variants did not emerge until 10 days after use of monoclonal neutralizing antibodies to spike protein.
Summary and conclusions:
To me to solve the issue of what contributes to poor VE of the COVID-19 vaccines requires that the correlates of protection are revealed. Sufficient evidence including the data in Image 1 implies innate immunity and not the IgG to spike protein is involved. It is not widely appreciated that neutralizing innate antibodies exist which do not recognize SARS-CoV-2 antigens which may clear pathogens.
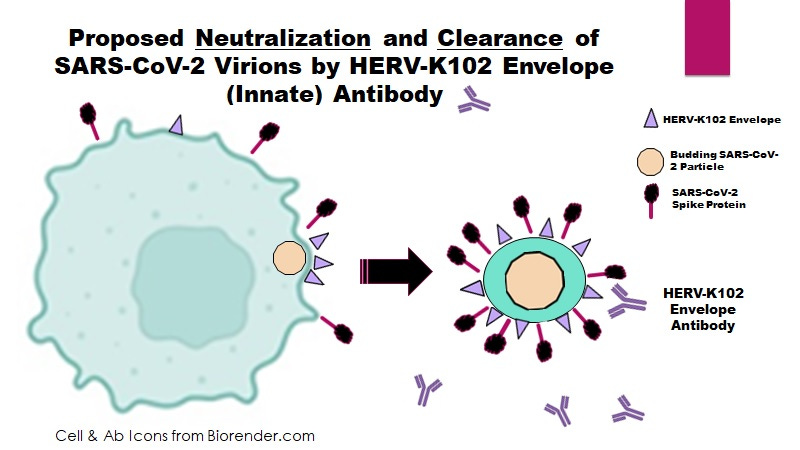
Image 8. HERV-K102 Envelope becomes expressed on virally infected cells and is incorporated into budding SARS-CoV-2 virions (as SARS-C0V-2 is an enveloped RNA virus). So antibodies to HERV-K102 envelope can clear and neutralize SARS-CoV-2 virions.
It is clear the mRNA C19 vaccines are toxic and promote coagulation, and myocarditis. They also likely promote immunosenescence at the level of the macrophage which inhibits both innate and adaptive immunity and thus, is very dangerous. Moreover immunosenescence causes chronic illness.
To me the story on imprinting is less clear especially given the data that the IgG to spike protein do not protect but cause progression to more severe COVID-19.
Refs
1. Zohar T, Alter G. Dissecting antibody-mediated protection against SARS-CoV-2. Nat Rev Immunol. 2020 Jul;20(7):392-394. doi: 10.1038/s41577-020-0359-5.
2. Chen W, Zhang J, Qin X, et al. SARS-CoV-2 neutralizing antibody levels are correlated with severity of COVID-19 pneumonia. Biomed Pharmacother. 2020 Oct;130:110629. doi: 10.1016/j.biopha.2020.110629.
3. Chen X, Pan Z, Yue S, et al. Disease severity dictates SARS-CoV-2-specific neutralizing antibody responses in COVID-19. Sig Transduct Target Ther 5, 180 (2020). https://doi.org/10.1038/s41392-020-00301-9.
4. Hashem AM, Algaissi A, Almahboub SA, et al. Early humoral response correlates with disease severity and outcomes in COVID-19 patients. Viruses. 2020 Dec 4;12(12):1390. doi: 10.3390/v12121390.
5. Zhao J, Yuan Q, Wang H, et al. Antibody responses to SARS-CoV-2 in patients with novel coronavirus disease 2019. Clin Infect Dis. 2020 Nov 19;71(16):2027-2034. doi: 10.1093/cid/ciaa344.
6. Shrock E, Fujimura E, Kula T, et al. Viral epitope profiling of COVID-19 patients reveals cross-reactivity and correlates of severity. Science. 2020 Nov 27;370(6520):eabd4250. doi: 10.1126/science.abd4250.
7. Choteau M, Scohy A, Messe S, et al. Development of SARS-CoV2 humoral response including neutralizing antibodies is not sufficient to protect patients against fatal infection. Sci Rep. 2022 Feb 8;12(1):2077. doi: 10.1038/s41598-022-06038-5.
8. Legros V, Denolly S, Vogrig M, et al. A longitudinal study of SARS-CoV-2-infected patients reveals a high correlation between neutralizing antibodies and COVID-19 severity. Cell Mol Immunol. 2021 Feb;18(2):318-327. doi: 10.1038/s41423-020-00588-2.
9. Ren L, Fan G, Wu W, et al. Antibody responses and clinical outcomes in adults hospitalized with severe coronavirus disease 2019 (COVID-19): a post hoc analysis of LOTUS China trial. Clin Infect Dis. 2021 May 18;72(10):e545-e551. doi: 10.1093/cid/ciaa1247.
10. Wang K, Long QX, Deng HJ, et al. Longitudinal dynamics of the neutralizing antibody response to severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection. Clin Infect Dis. 2021 Aug 2;73(3):e531-e539. doi: 10.1093/cid/ciaa1143.
11. Xu X, Nie S, Wang Y, et al. Dynamics of neutralizing antibody responses to SARS-CoV-2 in patients with COVID-19: an observational study. Signal Transduct Target Ther. 2021 May 18;6(1):197. doi: 10.1038/s41392-021-00611-6.
12. Gao L, Zhou J, Yang S, et al. The dichotomous and incomplete adaptive immunity in COVID-19 patients with different disease severity. Sig Transduct Target Ther 6, 113 (2021). https://doi.org/10.1038/s41392-021-00525-3.
13. Huang AT, Garcia-Carreras B, Hitchings MDT, et al. A systematic review of antibody mediated immunity to coronaviruses: kinetics, correlates of protection, and association with severity. Nat Commun. 2020 Sep 17;11(1):4704. doi: 10.1038/s41467-020-18450-4.
14. Nair S, Chen X. Biology of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and the humoral immunoresponse: a systematic review of evidence to support global policy-level actions and research. Glob Health J. 2022 Mar;6(1):38-43. doi: 10.1016/j.glohj.2021.11.005.
15. Zohar T, Loos C, Fischinger S, Atyeo C, Wang C, Slein MD, et al. Compromised humoral functional evolution tracks with SARS-CoV-2 mortality. Cell. 2020 Dec 10;183(6):1508-1519.e12. doi: 10.1016/j.cell.2020.10.052.
16. Tetro JA. Is COVID-19 receiving ADE from other coronaviruses? Microbes Infect. 2020 Mar;22(2):72-73. doi: 10.1016/j.micinf.2020.02.006.
17. Ricke DO. Two different antibody-dependent enhancement (ADE) risks for SARS-CoV-2 antibodies. Front Immunol. 2021 Feb 24;12:640093. doi: 10.3389/fimmu.2021.640093.
18. Moorlag SJCFM, Taks E, Ten Doesschate T, et al. Efficacy of Bacillus Calmette-Guérin vaccination against respiratory tract infections in the elderly during the Covid-19 pandemic. Clin Infect Dis. 2022 Mar 5:ciac182. doi: 10.1093/cid/ciac182.
19. Bigay J, Le Grand R, Martinon F, Maisonnasse P. Vaccine-associated enhanced disease in humans and animal models: lessons and challenges for vaccine development. Front Microbiol. 2022 Aug 10;13:932408. doi: 10.3389/fmicb.2022.932408.
20. Munitz A, Edry-Botzer L, Itan M, et al. Rapid seroconversion and persistent functional IgG antibodies in severe COVID-19 patients correlates with an IL-12p70 and IL-33 signature. Sci Rep. 2021 Feb 10;11(1):3461. doi: 10.1038/s41598-021-83019-0.
Ziegler CGK, Miao VN, Owings AH, Navia AW, Tang Y, Bromley JD, et al. Impaired local intrinsic immunity to SARS-CoV-2 infection in severe COVID-19. Cell. 2021 Sep 2;184(18):4713-4733.e22. doi: 10.1016/j.cell.2021.07.023.
Guerrieri M, Francavilla B, Fiorelli D, Nuccetelli M, Passali FM, Coppeta L, et al. Nasal and salivary mucosal humoral immune response elicited by mRNA BNT162b2 COVID-19 vaccine compared to SARS-CoV-2 natural infection. Vaccines (Basel). 2021 Dec 18;9(12):1499. doi: 10.3390/vaccines9121499.
Ren X, Wen W, Fan X, Hou W, Su B, Cai P, et al. COVID-19 immune features revealed by a large-scale single-cell transcriptome atlas. Cell. 2021 Apr 1;184(7):1895-1913.e19. doi: 10.1016/j.cell.2021.01.053.
Theobald SJ, Simonis A, Georgomanolis T, et al. Long-lived macrophage reprogramming drives spike protein-mediated inflammasome activation in COVID-19. EMBO Mol Med. 2021 Aug 9;13(8):e14150. doi: 10.15252/emmm.202114150.
Laderoute MP. A new paradigm about HERV-K102 particle production and blocked release to explain cortisol mediated immunosenescence and age-associated risk of chronic disease. Discov Med. 2015 Dec;20(112):379-91.
Jensen B, Luebke N, Feldt T, et al. Emergence of the E484K mutation in SARS-COV-2-infected immunocompromised patients treated with bamlanivimab in Germany. Lancet Reg Health Eur. 2021 Sep;8:100164. doi: 10.1016/j.lanepe.2021.100164.
I don't care what these papers say. The jab injected known poisons that depress the native immune system, create a system where by ALL your cells EVERYWHERE in the body express the spike. The spike is de facto a poison to the body and a clear and present danger. BUT. You've also dumped in SV40 (accelerant to turbo cancers) plus also other toxins (by using chemicals not cleared for human use), created a smoldering potential for prion (misfolding of proteins) disease longer term, and turned off expression of the DNA protective 'repair' proteins. Your body is now fixed in one direction ONLY and can't do anything to fend off any other insult. Result: poor health, and many other 'systemic' diseases flourish leading to? Excess mortality. Cut through the scientific blather of WHY. The shots are poison. Stop the shots. Stop the technology IT WILL NOT WORK. IT DOES NOT WORK. No more mRNA injections which are riddled with poor quality control, contaminants and are deadly to many. Yet, they are doubling down for mRNA shots in EVERYTHING. Your pets, your food sources the environment.
The conclusion thus is inescapable: THEY WANT YOU DEAD. The elites want you dead. The gov't controlled by the elites want you DEAD. A few scant of these 8,500 richest people in the world who govern you will also bite the dust, but that's just 'collateral'. Because honestly you don't think THEY ARE getting such 'required to live work etc' jabs? Nooo no indeedy not. They get the saline, they get a 'pass' they get 'clean food and water'. No dioxin contamination for them. I think you will find it doesn't matter the science. While you are busy arguing it, they are busy enforcing people taking it and those people are dying. SEE WHO Treaty please for a comprehensive look at your slavery ...
Thank You, Dr. Laderoute, for teasing out this complex mechanism of spike-protein immunosuppression.
"It may be the induction of immunosenescence by spike protein which drives the non-COVID-19 and COVID-19 associated excess mortality in the vaccinated over the non-vaccinated."