

I don’t think this is a case of healthy vaccinee bias.
I don’t think this is a case of healthy vaccinee bias.


The new immunosenescence paradigm of macrophages (Laderoute 2015).
The new immunosenescence paradigm [1] explains under what circumstances trained immunity (redefined as the induction of foam cell formation by HERV-K102 particle production in macrophages, Laderoute submitted [2]) can promote diseases (infectious and non-infectious); ie., when the HERV-K102 protector particles are not released.
It also attempts to explain how stress (elevated cortisol) and/or aging (diminished youth hormone, dehydroepiandrosterone (DHEA)), when out of balance (reduced DHEA/cortisol ratios), places the host at risk of immunosenescence. High cortisol induces alpha-fetoprotein expression, while low DHEA (a hormone that binds and inactivates AFP) means more AFP is active [1].
Since trained innate immunity induces ACE expression during the activation of macrophages, but which persists when the apoptosis of the foamy macrophages is blocked by active alpha-fetoprotein (AFP), it is believed that a sign of IMMUNOSENESCENCE (of macrophages) is hypertension beyond 7 days.
IMMUNOSENESCENCE means the macrophages are dysfunctional [1]: they are immunosuppressed and paradoxically also release the pro-inflammatory factors TNF-alpha, IL-6 and, IL-1-beta in an uncontrolled fashion. Both immunosuppression and the inability to downmodulate the proinflammatory factors is due to the active AFP triggering the 67 kD AFP receptor expressed on the macrophages. This signal involves the PI3K/Akt/mTOR pathway which bestows a malignant phenotype on the macrophages. AFP triggering the 67 kD AFPr generates a NEGATIVE signal which ABOLISHES ANY INCOMING SIGNAL. These macrophages are completely dysfunctional and unable to respond to signals properly.
To reverse immunosenescence which causes chronic diseases and is associated with acute failure to handle infections and tumors, one cannot use anti-inflammatories because they only serve to contribute to the pre-existing immunosuppression. Only AFP antagonists like zinc, flavonoids, DHEA (but preferably 7-keto-DHEA analogues which cannot be converted to other hormones such as male hormones in women) or even ivermectin [3] can counteract the effects of AFP.
DHEA (the anti-stress youth hormone) binds and renders AFP inactive [1]. In the elderly and/or stressed, there may be insufficient levels of DHEA compared with cortisol so the elderly are at higher risk of immunosenescence and thus, also at higher all-cause mortality including infectious diseases like COVID-19.
In a recent correspondence to the New England Journal of Medicine, Hoeg et al [4] suggested that a significant lowering of non-COVID-19 mortality in an observational study due to a booster shot [5] was not possible and argued there must have been ‘healthy vaccinee bias’. They estimated a difference of 95 %, but the actual observed was 77% [6].
The notion that trained innate immunity (TI) can generate significant heterologous protection against infectious agents and tumors is not disputed [7].
What may be conceptually new is that the induction of TI also reverses chronic diseases. In other words, a potent signal for TI induction can overcome the blocked signal of TI referred to as IMMUNOSENESCENCE OF MACROPHAGES (see above).
It has been recently demonstrated by Yamaguchi et al [8], that the Pfizer BioNTech mRNA vaccine induces trained innate immunity which is even enhanced by the second dose (temporarily). The differentially expressed genes (DEGS) of trained immunity when combined together provided a signature in the monocytes tested in blood. This signature was down-regulated in patients who progressed to severe COVID-19, showing TI protects against COVID-19. The loss of TI in the patients with severe COVID-19, likely occurred because of antibody dependent enhancement (ADE) of infection of SARS-CoV-2 into the foamy macrophages by the spike specific IgG1/3 [2].
Thus, it was not surprising that studies published in the CDC journal MMWR demonstrated COVID-19 vaccines were in fact able to decrease non-COVID-19 mortality when compared with the unvaccinated [9]. For example, for non-COVID-19 mortality in the vaccinated over the unvaccinated (1 or 2 doses) for a period covering up to the end of July 2021 (ie., notably before delta); a hazard ratio (HR) of about 0.3 was reached for ages 45-84 with either the Pfizer BioNTech or Moderna mRNA vaccines [9]. Thus, the objections by Hoeg et al [4] that this level of heterologous protection was impossible appear to be unfounded.
However, the promotion of TI by mRNA vaccines however has its dangers because at 28 days after the second dose of BNT162b2, TI was completely aborted [8]. So if anything was wrong, the original study by Arbel et al [5] was kept short (54 days) to minimize the loss of TI benefit in order to show the boosters improved outcomes.
Allegedly, it seems that there may have been some fudging of data [5] which of course would favor the enhancing of the benefits related to having received a booster shot. It it appears that for anyone who got infected at up to 3 days after being boosted, this data (1020 participants) was entirely excluded from the analysis [5]. Plus, anyone infected from 4 days to 7 days after boosting was lumped in the control group ( how many?), so any associated deaths that occurred later would be associated with the control group.
Since 9/10 participants served as the control until boosted means there was no or little introduction of healthy vaccinee bias, lending little substantiation to the complaints expressed by Hoeg et al [4].
HOWEVER, if we look at Table 1 (Image 1) for participant characteristics
[https://www.nejm.org/doi/full/10.1056/NEJMoa2115624],
we can see that following the booster dose an excess of 28,681 persons (8%) developed hypertension due to the 3rd dose, so if anything the risks of death became elevated once the participant was boosted. Hypertension (beyond 7 days) is a sign of immunosenescence [1,2] so it enables us to follow the loss of heterologous protection afforded by TI which incidentally, would adversely affect non-COVID-19 mortality. There was no “clinically significant” increase in any of the other risk factors despite claims that a 1% increase was statistically significant.

Image 1. Characteristics of Study Participants from the Arbel R et al 2021 NEJM paper [5][https://www.nejm.org/doi/full/10.1056/NEJMoa2115624].
If we look at the hazard ratio (HR) for non-COVID-19 versus COVID-19 mortality (Image 2) we see that generally the risk factors greatly impacting for COVID-19 severity and death are generally not shared by those risk factors for non-COVID-19 mortality where for the latter the risk is often less (see male sex and chronic renal failure on the left panel versus the right in Image 2). However, we note that the boosted have much higher risks of non-COVID-19 related lung cancer death (left side panel HR is higher than the right side panel). Given that the incidence of hypertension was the only risk factor that increased after being boosted (Image 1), I would hazard a guess that the risk for hypertension related non-COVID-19 deaths would have also substantially increased. Given that hypertension is a well-known and well established risk factor for COVID-19 severity and death, one can only imagine why Arbel et al, neglected to list it in their analyses.
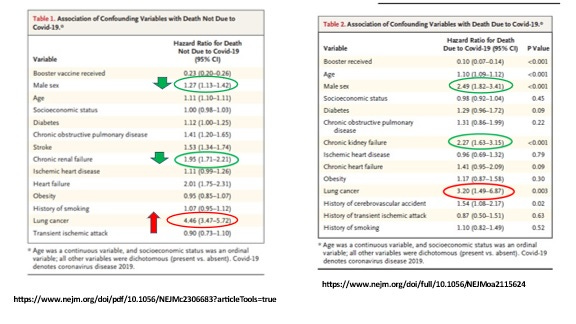
Image 2. Lung cancer NON-COVID-19 death rates skyrocketed upon the booster dose. What about hypertension?
So today, I requested this missing information on hypertension from the lead author, Dr. Ronen Arbel as well as information on what the data would look like if the 1020 excluded SARS-COV-2 infections in the boosted were included in that group along with any other infections that occurred up to 7 days. [It makes no sense to exclude these when examining non-COVID-19 mortality]. I have also requested an analysis of the data over a longer period of time such as at 4 months.
We know that for the MMWR data [9] the authors purposefully chose a period of time (December 14, 2020 to July 31, 2021) prior to the dominance of the delta variant as the benefits on non-COVID-19 mortality would have plummeted due to ADE which associates with the selection of variants by mass vaccination [2].
As shown in Image 3 for excess non-COVID-19 mortality in the UK stratified by age and sex [10], heterologous protection by the mRNA vaccine (green area) was dominant in the 50 plus age group during this time (December 2020 to May/June in 2021 as reflected in the negative excess non-COVID-19 mortality. The vast majority of UK citizens over 50 received one dose of vaccine during this period (data not shown).
However, with time from July to December 2021, there is an increase in excess non-COVID mortality associated with the establishment of the delta variant. This implies through ADE that there was a loss of trained immunity that becomes quite notable in the 50 to 64 year old age group. This group is not normally at higher risk of death so the change by the delta variant is quite different that the years from 2015-2019. However there is a reprieve during the first 4 months of 2022 for the 65+, but not for males under 25 who were at excess risk of non-COVID-19 mortality.
Most citizens in the UK over the age of 50 had received the 3rd dose of vaccine from October to December 2021. This may have also helped to lower the risk of non-COVID mortality in the first 4 months of 2022 via induction of trained immunity in addition to omicron doing the same.
As discussed in a previous post, following the third dose, the spike specific IgG1 and 3 which cause ADE are converted to IgG4 which does not mediate ADE. However, most citizens would have been infected by omicron and this natural infection apparently could affect this conversion process.
From June 2022 to December 2022 we see across all ages a notable increase in excess non-COVID-19 mortality. The omicron variants are known not to cause COVID-19 pneumonia. However, by the third or fourth doses of mRNA injections, the toxicity of the mRNA gene therapy vectors becomes quite evident.
Image 3. UK Excess Non-COVID-19 Mortality By Age And Sex For March 2020 Through May 2023 Shows In The 50 + There Was A Significant Period Of Negative EXCESS Non-COVID-19 Mortality For The Period Covering December 14, 2020 To June 31, 2021. [10]
In conclusion, the potency of the induction of TI on reducing non-COVID-19 mortality can be tremendous. It may be somewhat surprising to clinicians that mRNA vaccines, by inducing trained immunity may even reverse cardiovascular and other common forms of chronic disease in recipients.
This means the public can look forward to the day that ‘disease care’ transitions to ‘health care’ where instead of using anti-inflammatories (which only perpetuates disease by treating the symptoms) one uses AFP antagonists to cure disease by targeting the cause of chronic disease…IMMUNOSENESCENCE.
We should not be swayed by (allegedly) manipulated data captured in a small window of benefit of the COVID-19 mRNA vaccines when the landscape clearly spells far greater trouble ahead for the COVID-19 mRNA vaccinated, as shown for all age groups in Image 3. IN COMPARISON TO PREVIOUS YEARS the data in Image 3 clearly shows that the under 25 were not in any big trouble with the pandemic… that is, until they became vaccinated.
Laderoute M, Discovery Medicine 2015.
Laderoute M, Trained immunity involving HERV-K102 activated in foamy macrophages may promote recovery from COVID-19 providing a new innate immunity vaccination paradigm against pandemic RNA viruses. (submitted invited review, July 31, 2023).
Laderoute M. Ivermectin may prevent and reverse immunosenescence by antagonizing alpha-fetoprotein and downmodulating PI3K/Akt/mTOR hyperactivity. Open Heart. April 29, 2021. https://openheart.bmj.com/content/8/1/e001655.responses#ivermectin-may-prevent-and-reverse-immunosenescence-by-antagonizing-alpha-fetoprotein-and-downmodulating-pi3k-akt-mtor-hyperactivity.
Hoeg, TB, Duriseti R, Prasad V, Correspondence NEJM July 20, 2023.
Arbel R, Hammerman A, Sergienko R, Friger M, Peretz A, Netzer D, Yaron S. BNT162b2 vaccine booster and mortality due to COVID-19. N Engl J Med. 2021 Dec 23;385(26):2413-2420. doi: 10.1056/NEJMoa2115624.
Reply Arbel R et al, Correspondence NEJM, July 20, 2023.
Al B et al, J Allerg Clin Immunol June 14, 2023.
Yamaguchi Y et al, JCI Insight 2022; doi: 10.1172/jci.insight.163347.
8.
Xu S et al, MMWR, 2021 [https://www.cdc.gov/mmwr/volumes/70/wr/pdfs/mm7043e2-H.pdf].
based on the following UK excess non-COVID-19 mortality data: The UK Office for Health Improvements and Disparities (UKHID) released a downloadable database on June 8, 2023 [https://www.gov.uk/government/statistics/excess-mortality-in-england-and-english-regions] but where charts of the excess mortality data by month, sex and age were compiled and made available by Stuart A @OutsideAllan on twitter on June 8 2023.
Excellent attention to (the devil in the ) Details, Dr. Laderoute!
"So today, I requested this missing information on hypertension from the lead author, Dr. Ronen Arbel as well as information on what the data would look like if the 1020 excluded SARS-COV-2 infections in the boosted were included in that group along with any other infections that occurred up to 7 days. I have also requested the extension of the data over time such as at 4 months."
The 7 day hypertension looks very interesting. Can we propose a mechanism?
I didn't see any laboratory data in the original paper but it would have been nice to assess the chemistry in anyone who had new hypertension within the first week after the shot.
My first thought was spike protein damage to the renal arteriolar glomerular epithelium. Before and after creatinine might be a clue here.
Next I wondered about micro emboli and thrombi. D-dimer would help this proposal.
Antiphospolipid syndrome? (Mentioned in another Substack this month, not one of my strong points since stopping obstetric deliveries in 2002!}
In general hypertension progresses over some years as the patient and his arterial system ages and deteriorates, so a 7-day progression is significant. If you know Dr. Ellen Burgess in Calgary she has been an expert for decades. Did your request for data include clinical parameters or just the statistics shown in the supplement?
Thank you again for illuminating this aspect of immunology. Dr. Jessica Rose this weekend has posted a report of studies on the effect of thiols/cysteine on cellular immunity and spike interactions. I may soon understand more of the pathologic mechanisms involved in Covid and vaccine damage.