


Guessing at the Number of COVID-19 Shot Associated Deaths In CANADA
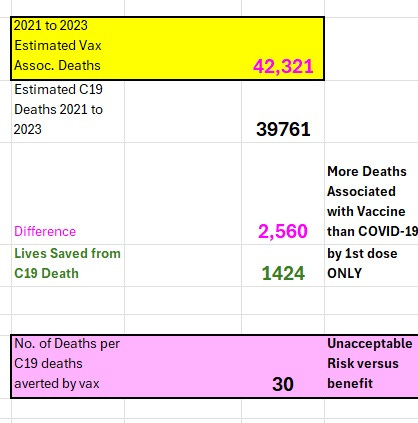
Governments do NOT want you to know that there were more deaths associated with the vaccines than COVID-19 and An Estimated only 1424 C19 Deaths were averted in 2021 due to the First Shot

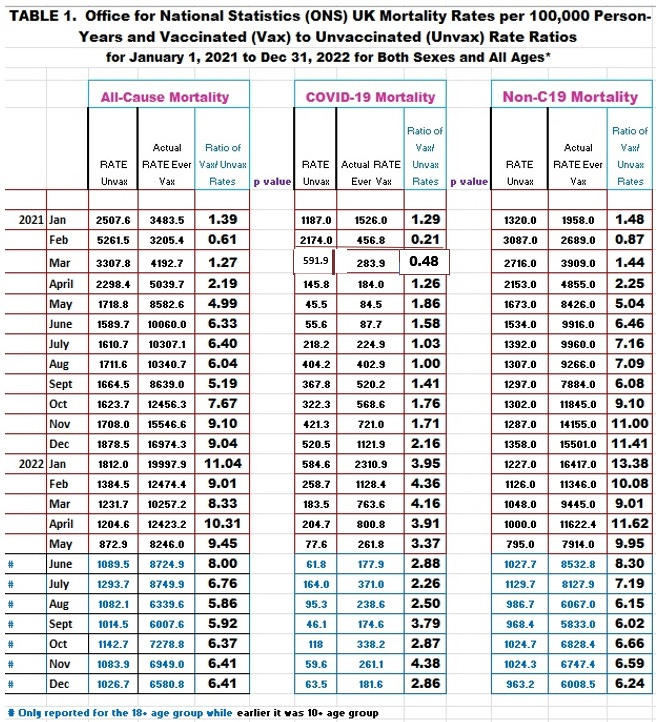
For taxpayers’ money, there is no reason why we need to be guessing at how many deaths were ACTUALLY associated with the vaccines and the total number of lives saved. How difficult is it to link the vaccination record with death certificates? The UK did it, so why not Canada or the USA? Of course there was some manipulation of the data in the UK (their summary statistics for the total rates for the unvaccinated apparently included all deaths that occurred during the first two weeks of receiving a shot according to Professor Norman Fenton) but recompiling the results (adding up all the rates in each of the vaccination categories) revealed the expected pattern for a vaccine that was neither safe nor effective (Table 1).
This pattern shown in Table 1 for the UK entire population data indicates a favorable all-cause mortality was ONLY reached in February 2021 but not in any other month. This represented a period of time where about 96 % of the elders (who have the highest risk of death) had only had the first shot (promoting the life-saving HERV-K102 trained (innate) immunity). This directly proves that it is the second shot which induces the IgG1/3 to spike protein THAT IS DEADLY!
Indeed the C19 vaccines should have been globally withdrawn by the first week in February 2021 had the factual unmanipulated data been transparently released in REAL TIME by the UK.
The problem with the ADAPTIVE IMMUNITY C19 vaccines is due to antibody dependent enhancement (ADE) of infection into macrophages which destroys the critical immunity called “trained innate immunity” (involving HERV-K102 activation) in macrophages.
This defense system is CRITICAL BECAUSE IT preserves human life OF THE INDIVIDUAL AND PUTATIVELY, THE Homo sapiens SPECIES [Laderoute M, Preprints, 2023].
To read more about this NOVEL and magnificent “virus anti-virus system” of macrophages unique to humans targeted by ADE you are invited to examine a recent preprint article:
Laderoute, M. Antibody Dependent Enhancement (ADE) of Infection into Macrophages Validates the Importance of HERV-K102 Particle Production for Pandemic Preparedness. Preprints 2023, 2023120185. https://doi.org/10.20944/preprints202312.0185.v1
From the get-go, everybody knew that the adaptive COVID-19 vaccines by inducing IgG1/3 antibodies to the spike protein would be a disaster because during natural infection these antibodies cause progression to severity including DEATH by ADE [reviewed in Laderoute M, 2023]. In other words, these antibodies do not protect but hinder protection.
As discussed before, ADE causes progression according to this schematic (Image 1) which essentially knocks out trained innate immunity of lipid body negative foamy macrophages (LB-FMs). The LB-FMs are the main cells in the body which produce and release the protector HERV-K102 foamy virus particles.
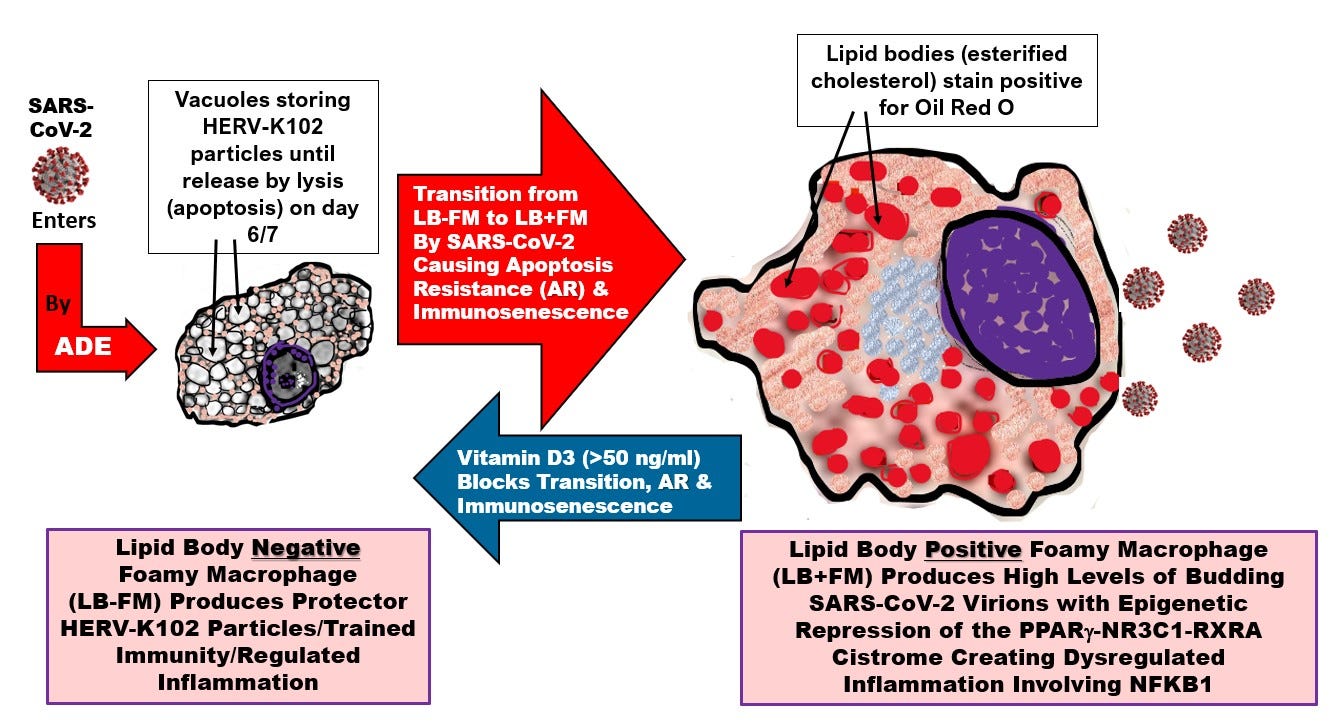
Image 1. ADE knocks out critical host INNATE immunity defenses of the LB-FMs and produces immunosenescence of the macrophages which causes chronic disease.
Why ADE is Dangerous
The lipid body positive foamy macrophages instead churn out high levels of SARS-CoV-2.
In total, ADE causes :
crippled trained innate immunity so immunosurveillance against cancers and pathogens is weakened (the former likely contributes to ‘turbo cancers’),
induction of immunosenescence of macrophages which causes hypertension, heart disease, tumors & ‘turbo cancers’, insulin resistance, autoimmune disease, neurodegenerative disorders, etc., and
a safe haven for the high reproduction of SARS-CoV-2 variants
which act together to cause progression to severe COVID-19 and increase the likelihood of death (unless your levels of vitamin D are well over 50 ng/ml which blocks the deadly transition to immunosenescence).
There are two types of foamy macrophages which has over the past 4 decades obfuscated the study of atherosclerosis and cardiovascular disease (CVD) which generally does not distinguish these two very different cell types shown in Image 2.
Image 2A) foamy macrophages are associated with health while Image 2B) foamy macrophages are associated with disease, in this case tuberculosis.
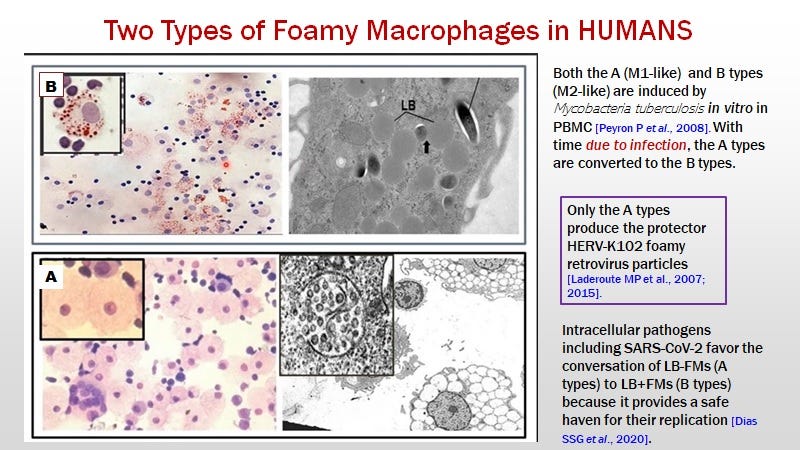
Image 2. Two Types of Foamy Macrophages A) associated with health and Image 2B) associated with disease, in this case tuberculosis.
I have defined immunosenescence of macrophages as the failure to release HERV-K102 particles by lysis from the type A foamy macrophages (the LB-FMs) [Laderoute M, Discovery Medicine 2015 and 2020] (Image 3). Often immunosenescence occurs by pathogen-mediated transition to the lipid body positive foamy macrophages (Image 2B)
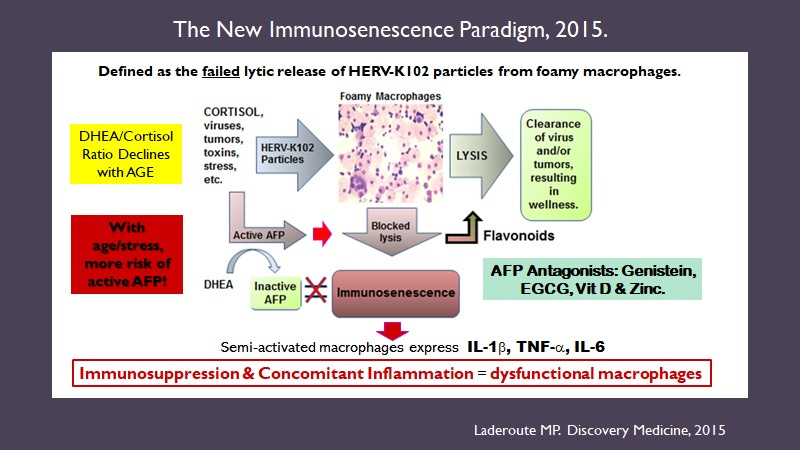
Image 3. Immunosenescence of Macrophages Causes Chronic Diseases (cancers and infections due to loss of the critical HERV-K102/trained innate immunity needed for immunosurveillance and CVD, autoimmune conditions, neurodegeneration etc., via deregulated release of pro-inflammatory factors such as IL-1beta, TNF-alpha and IL-6).
NB: Agents that prevent or reverse immunosenescence are alpha-fetoprotein (AFP) antagonists such as flavones (genistein, EGCG), zinc, vitamin D (likely indirect) and now ivermectin [Laderoute M, 2021].
Laderoute M. Ivermectin may prevent and reverse immunosenescence by antagonizing alpha-fetoprotein and downmodulating PI3K/Akt/mTOR hyperactivity. Open Heart, April 29, 2021. https://openheart.bmj.com/content/8/1/e001655.responses#ivermectin-may-prevent-and-reverse-immunosenescence-by-antagonizing-alpha-fetoprotein-and-downmodulating-pi3k-akt-mtor-hyperactivity
Inflammation per se Does not cause Disease: It is immunosenescence caused by alpha-fetoprotein (AFP)
We found in our Immune System Management (ISM) clinic which re-established wellness in patients with serious and often severe diseases (largely advanced cancer patients) by reversing immunosenescence (since 1998 generally and since 1992 in patients with advanced breast cancers), that most anti-inflammatories such as statins, turmeric, or melatonin >2 mg per night, prevented the re-establishment of wellness.
I personally witnessed this when I was Lab and Research Director at ISM (Ottawa, Canada) from 2011 to 2020 as I monitored the state of their innate immune system with several proprietary algorithms concerning the amino acid profile that were in fact validated by clinical outcomes!
In other words most anti-inflammatories are in fact, immunosuppressive and prevent the induction of HERV-K102 particle production in foamy macrophages as shown in Image 2A. One can only prevent and reverse immunosenescence by using proven AFP antagonists. Apparently, dexamethasone inhibits HERV-K102 activation while methylprednisolone seems to activate it. This may be why methylprednisolone is favored by the FLCCC over dexamethasone in their treatment of severe COVID-19!
Lets Look at the Causes of Death During the Pandemic for Canada
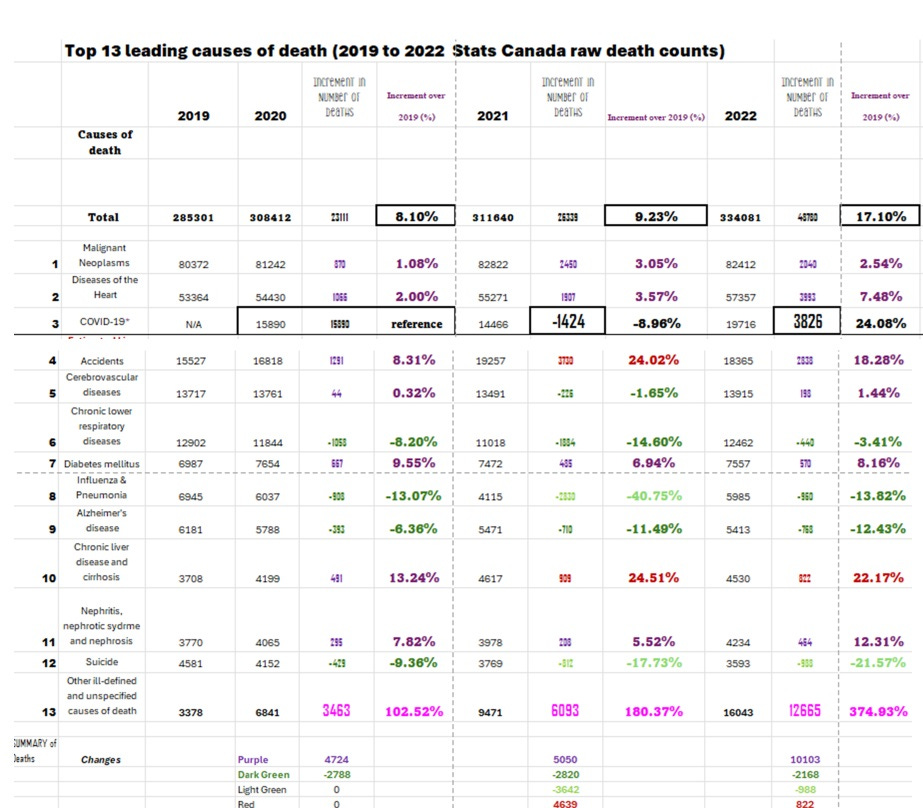
Image 4. Changes in the Top 13 Causes of Death over the Pandemic Years.
Some causes increased (in purple) and some really increased over 20% (in red). Others decreased (in dark green) and others decreased quite a bit (light green). Suicides went down while accidents went up. The increased liver disease is likely due to excess AFP activity as well.
Category 13 “Other ill-defined and unspecified causes of death” were taken to represent ‘sudden deaths’ which appear to be promoted somewhat by SARS-CoV-2 infection (in the year 2020) but also increased associated with the COVID shots in 2021 and EVEN further with boosters by 2022. These deaths are represented by the hot pink color.
Note the almost 400 % increase in 2022 over 2019 for unspecified causes of deaths (hot pink stats)!
(WOW)
Calculation of the Number of Deaths Associated with C19 Vaccine-Induced Immunosenescence by Year for Canada
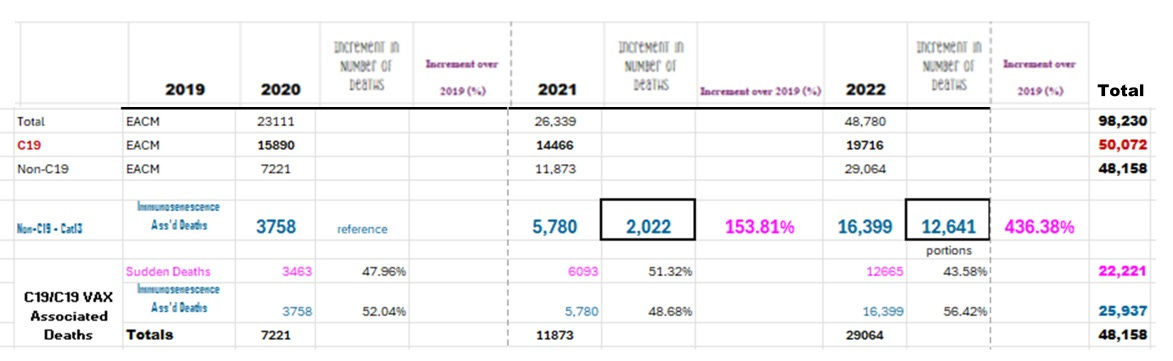
Image 5. Calculation of the Number of Deaths Associated with C19 Vaccine-Induced Immunosenescence by Year for Canada
Although technically COVID-19 deaths also involved immunosenescence, the non-COVID-19 deaths were considered to involve both the direct toxicity of the vaccine (injection into bloodstream and induction of pulmonary emboli, as well as clots and myocarditis/pericarditis) and immunosenescence causing chronic diseases like hypertension, CVD, cancers, turbo cancers, autoimmune diseases, neurodegenerative diseases, metabolic syndrome and insulin resistance, etc.
So to calculate the number of immunosenescence deaths per year associated with C19 vaccination in Canada (Image 6): the algorithm is described in Image 7.

IMAGE 6. Estimates that Excess Immunosenescence Deaths in Canada (Over 2020 Levels ) Caused by the mRNA COVID-19 Vaccines (two or more doses ) Worsened with Each Booster and Could Explain in part the Higher Risks of non-C19 Deaths in the Vaccinated Over the Unvaccinated Demonstrated for the UK (Table 1).
Note however, in Table 1, the relative risks of death in the vaccinated over the unvaccinated also include the toxicity of spike protein in the vaccine which causes sudden death so the ratios in Table 1 for the UK were expected to exceed the predicted impact of immunosenescence calculated for Canada.
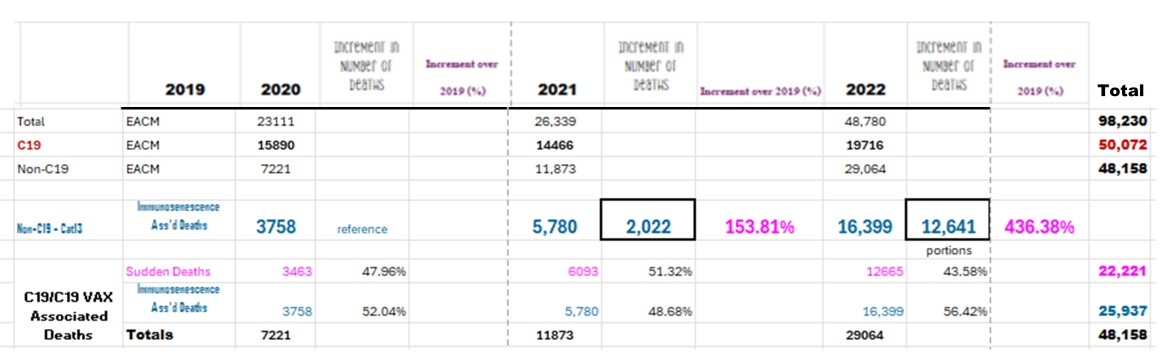
Image 7. To calculate the excess number of deaths due to immunosenescence, I took the excess all-cause mortality by year and subtracted the C19 deaths (note immunosenescence also causes influenza and pneumonia deaths) which left a parameter called non-COVID-19 deaths (Non-C19). From this I subtracted the Sudden Deaths equated with the 13th category of cause of death that escalated during the pandemic. This left me with an estimate of the number of NON-C19 deaths associated with immunosenescence of Image 6.
The ages of those dying during the pandemic may provide clues to mechanisms.
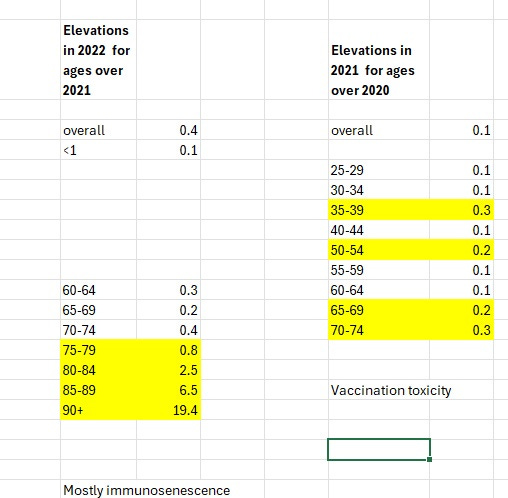
Image 8. According to Stats Canada the increase in mortality rates in Canada featured different age groups in 2021 over 2020 and for 2022 over 2021 implying different mechanisms of pathology. During active immunization with the ‘clot shots’ in 2021 we see that younger age groups are affected along with older age groups while in 2022 it is mainly the elder population (which also were the ones most often taking booster shots). The risk of immunosenescence increases with age [Laderoute M, 2015, 2020].
https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310039201
Other Points of Interest
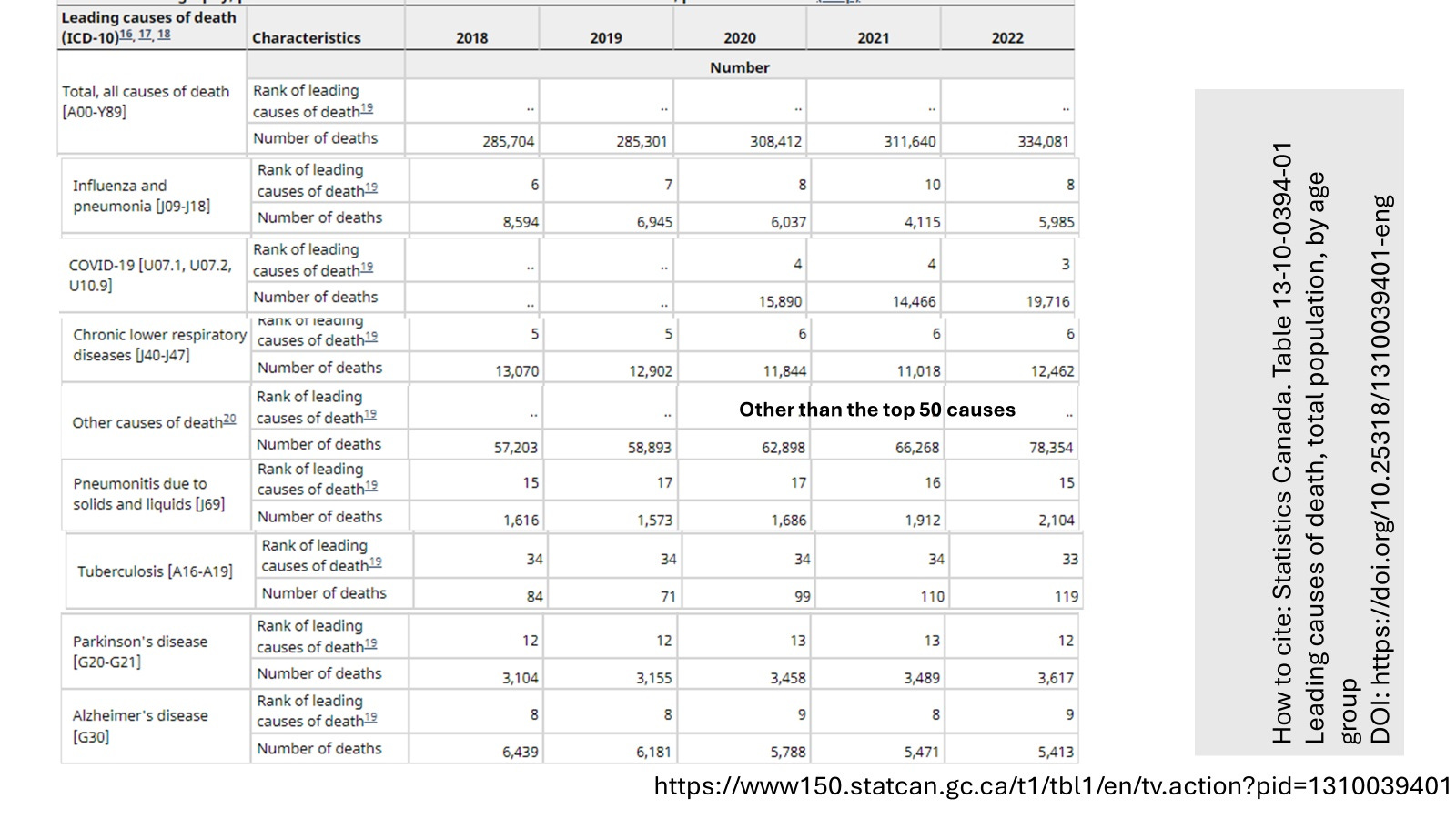
Image 9. COVID-19 Infections DID not cause influenza and pneumonia deaths to disappear in Canada.
This was a concern of some for the USA data
https://twitter.com/I_Am_JohnCullen/status/1741884103073694204
and where it was on the other hand argued that excess mortality peaks in the USA correlated with peaks in Influenza and pneumonia. This then supposedly casted doubts as to whether vaccines were causing excess mortality peaks.
But if the vaccines were largely causing deaths by immunosenescence, all peaks of infections (C19, RSV, influenza, pneumonia, Mycobacteria and bacterial infections) analyzed together or separately would be expected to correlate with excess all-cause mortality. So the arguments by John Cullen that the majority of all-cause mortality peaks in the USA correlated with the levels of influenza and pneumonia (in fact accounting only for about 20% or less of the USA deaths during major all Cause mortality peaks) does not invalidate the notion that vaccination damages the innate immune system which then increases the risks of death by infections but also chronic diseases, both by immunosenescence.
The analysis is further complicated by the fact that the first dose strongly induced trained (innate) immunity which diminished all-cause mortality and even generated negative excess mortality from Feb 10, 2021 to April 28, 2021 in Canada (Image 10). It is this trained innate immunity that gave the favorable results in the UK but only for the month of February 2021 (Table 1).
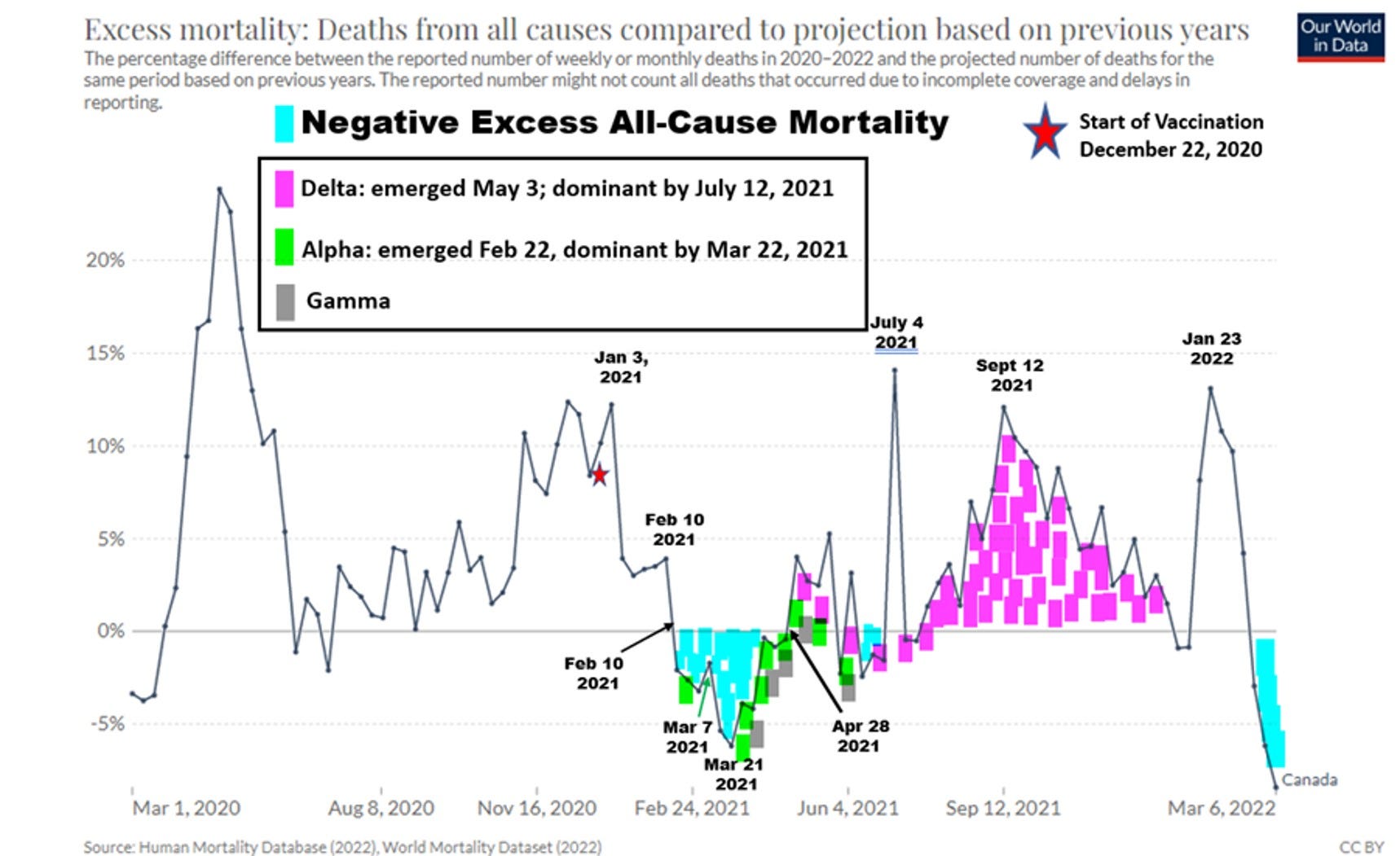
Image 10. The first dose of mRNA vaccines induced a reduction in EACM (Jan 3 through April 28, 2021 in Canada) while the second dose caused the emergence of the Delta variant which then corresponded with enhanced all-cause mortality [Laderoute M, 2023].
The July 4, 2021 peak in Canada related to over 600 heat related deaths in the province of British Columbia and should be ignored (Image 10).
The emergence of the omicron variant (highly mutated spike protein) in December 2021 caused an increase in excess all-cause mortality (EACM) despite the lack of lower respiratory tract pathology characteristic of earlier SARS-CoV-2 variants. However, by January 23, 2022, interestingly omicron exposure thereafter reduced EACM (Image 10).
This can be taken to mean omicron infection caused immunosenescence associated deaths in i) people with pre-existing immunosenescence (those with comorbidities including hypertension, cancer, CVD and diabetes) and ii) people double or triple vaccinated who had low or inadequate levels of vitamin D3 (see Image 1). On the other hand, in unvaccinated people with adequate levels of vitamin D, the omicron exposure acted like an innate immunity vaccine which then reduced excess all-cause mortality in part by reversing immunosenescence. This benefit may have also been the case in double or triple vaccinated individuals but who had optimal levels of vitamin D3 (see Image 1).
Note that trained innate immunity only lasts about 6 months. Since it is the trained innate immunity providing protection against death, this is why the public health officials were saying to get boosted every 6 months!
That vaccination and SARS-CoV-2 exposure history affects COVID-19 severity risks such as for the delta and omicron variants was recently shown by Uuskula A et al, [Scientific Reports, 2023]. The details are somewhat complicated and will not be discussed here.
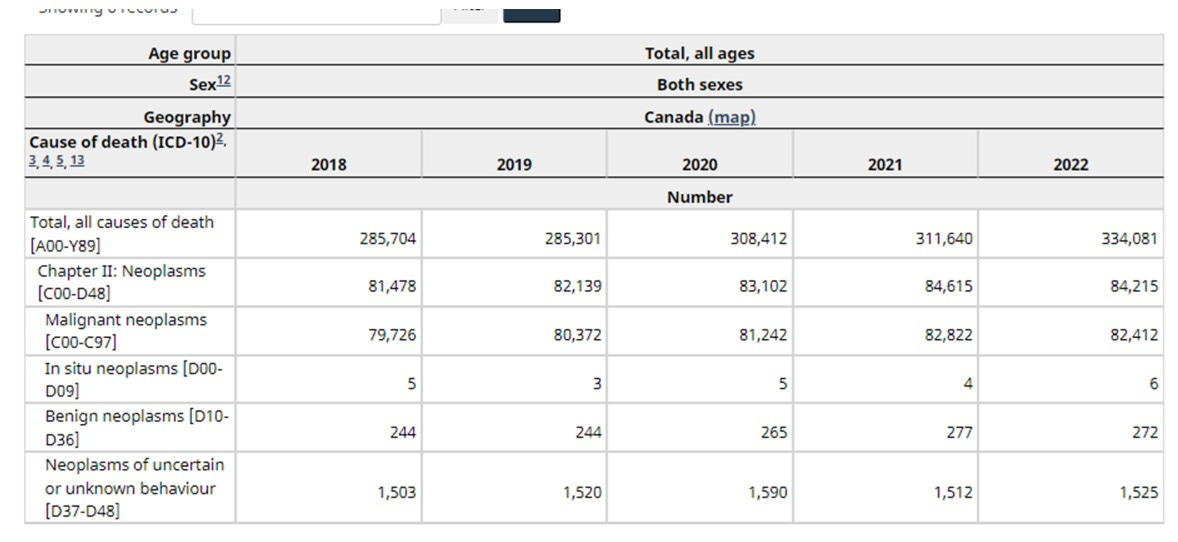
Image 11. No significant increases in cancer deaths (ie., not above 5 % increase over previous year) noted for 2021 and 2022 in Canada.
Despite reports of turbo cancers in 2022 in Canada, the total level of cancer deaths did not rise in 2022. It will be interesting to see what analysis of 2023 reveals.
CAVEAT for why vaccination associated deaths in Canada may be proportionately less than other nations such as the USA or UK
Using Excess All-Cause Mortality (EACM) to estimate the number of deaths associated with mRNA COVID-19 shots underestimates when compared to actual numbers such as reported by the UK ONS.
For example Jan 1, 2021 up to May 31, 2022 the EACM method predicts about 30,000 Vax Associated deaths in Canada while the algorithm prorated from UK ONS data suggests over 250,000 vax associated deaths in Canada to end of May 2022.
However, the data reported in Images 4 and 9 for total excess mortality over 2021 and part of 2022 for Canada limits the maximal number of excess deaths from 2021 and until May 31, 2022 at about 47,064.
Why then might Canada suffer less vaccination induced deaths than the UK or the USA?
There may be several reasons for this. First Canada’s median age of the population may be lower than the USA or the UK.
However Canada’s median age is 41.8, the UK is 40.6 and the USA is 38.5 [https://www.worlddata.info/average-age.php]. Canada has the highest median age. So this cannot explain why Canadians were not as hard hit by the COVID-19 shots.
Perhaps due to a better health care system in Canada and other aspects of health (less obesity than the USA), Canada may have a longer life-expectancy. This seems to be the case: Canada’s life-expectancy is 82.7 years, the UK is 80.8 years and the USA is 76.4 years [https://www.worlddata.info/average-age.php].
Fewer Canadians may have been vaccinated than the USA and the UK. However, the data reveals that Canada had the highest C19 shots per 100 people overall but that the UK had the highest number of 3rd shots (Image 12). The ONS UK data did show that the bulk of the mortality risk related to the third shot.
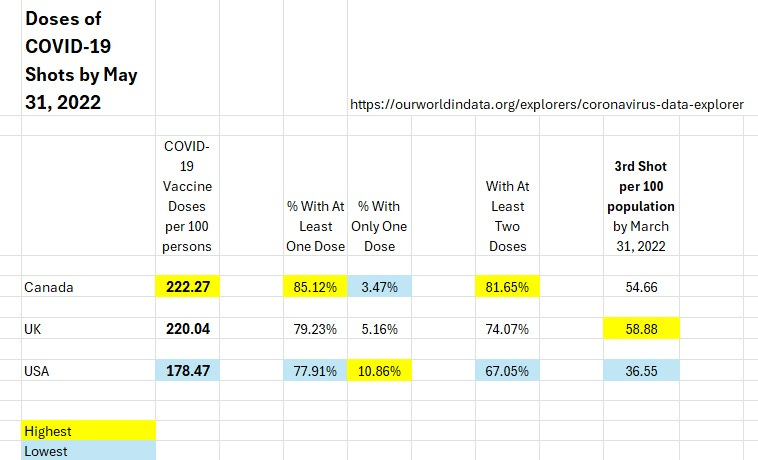
Image 12. Canada had the highest level of COVID-19 shots but the UK had slightly higher number of third shots (which according to the ONS data were more deadly).
An alternative explanation for why the UK exhibited higher death rates associated with vaccination than Canada could have related to a SECRET reason that few know about.
The overestimation for Canada could be if the UK received and administered more bad lots of the Pfizer C19 vaccine than Canada.
Canada has a history of lot release at Health Canada for biologics which forces manufacturers to put their best lots forward to Canadians. For example during the heparin contamination with oversulfated chondroitin sulfate in 2008 which caused about 150 deaths in the USA (due to shellfish allergies), at the time of HC testing there was only one small batch that got through to Canada (was this a test lot by the manufacturer?) while many if not most lots in the USA were contaminated.
As a LEGAL side note, if Pfizer provided Canada with safer lots (if true) shows Pfizer knew about the existence and dangers of the contaminants in its COVID-19 gene therapy shots.
So in summary:
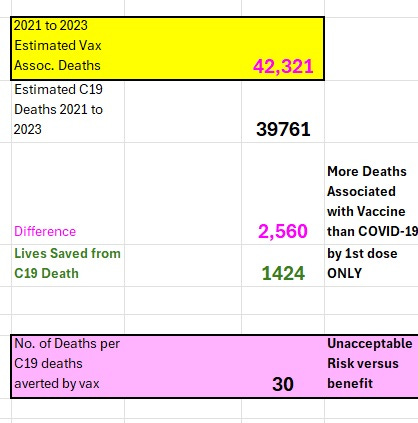
Image 13. For each COVID-19 death averted by COVID-19 vaccines (up to end of 2023), there were about 30 C19 Vaccine Associated Deaths.
There were only 1,424 deaths saved by vaccination which would have been due to trained innate immunity induced by the first dose and prior to the second dose. For each dose of C19 vaccine that saved a life from COVID it is estimated 30 additional Canadians died.
This is why safety and efficacy assessments MUST always examine all-cause mortality (like the leftmost column in Table 1).
What good would it be to cure one disease but in doing so increases the risk of dying from another disease and in more individuals??
Being vaccinated with at least two doses increased instead of decreasing infection/transmission and overall risk of death (Table 1) [Laderoute, M, 2023].
Being vaccinated with two doses did not save Granny, but may have placed her at higher risk of infection and subsequently all-cause mortality.
Being vaccinated increased the risk of toxicity (pulmonary embolism, sudden deaths, clotting, myocarditis/pericarditis) and increased the risks of immunosenescence (Image 5) the latter which became exacerbated over time with more SARS-CoV-2 exposures and vaccine exposures. Don’t forget these vaccines increased the risks of being SARS-CoV-2 infected (remember the Cleveland Clinic data?).
Clearly the government is keeping this important and definitive mortality data secret so that you don’t know or realize they put your life on the line without your knowledge or permission.
I would also like to warn about the use of hypericum (St. John's wort). While hypericum blocks insomnia, fatigue and brain fog, it seems to do this via inhibiting HERV-K102 particle production in vivo [Laderoute MP. Clues to finding correlates of risk/protection for HIV-1 vaccines [version 2; peer review: 2 approved with reservations] F1000Research 2018, 6:868 https://doi.org/10.12688/f1000research.11818.2. ]. That is to say that I was on hypericum for my chronic fatigue syndrome (zero HERV-K102 particles per ml of plasma) and upon dechallenge (stopped the therapy) at 84 hours I had 2.55 x 10 (11) particles per ml of plasma (proven to be cDNA and not genomic DNA). Hypericum also blocks HERV-K102 particle production in vitro (unpublished data). While Z-DTOX [zstacklife.com] does not contain anything that blocks HERV-K102 particle production, the so called Z-SHIELD contains both St. John's wort and turmeric which block HERV-K102 particle production. I think Dr. Mary Bowden (twitter @MDbreathe) indicated that for Post- C19 Vax Sequelae (PVS) she first starts with ivermectin and sees how the patient does. Then she uses the Z-DTOX. As far as I understand it, she does not recommend high dose melatonin (over 2 mgs) nor any turmeric. Resveratrol is another ingredient that seems to block recovery/HERV-K102 particle production and should be avoided in my opinion. For the respite from the insomnia, fatigue, and extreme brain fog, I now use NuSleep (ISM Ottawa, Canada) along with whey protein, one a day vitamins, fish oil (1800 EPA and 1000 DHA) and the equivalent of Z-DTOX (except I use genistein/flavones 60 mg instead of EGCG 100 mg). In the summer I try to be outdoors for at least one hour per day to reap the benefits of Vitamin D3 and near infrared. Last year I took up pickleball.
This is such an important question. Allopathic medicine and natural medicine commonly use anti-inflammatories to treat chronic diseases to little or no avail. This approach never cures diseases because they are only treating the symptoms. But the cause of chronic diseases (including cancer, CVD etc) is the immunosenescence of macrophages due to the activity of alpha-fetoprotein (AFP). So to cure chronic diseases one must use DIRECT AFP ANTAGONISTS LIKE IVERMECTIN, ZINC, FLAVONES, 7-KETO-DHEA and indirect like vitamin D3 blood levels at >50 ng/ml. Many if not most anti-inflammatories are immunosuppressive and block the activation of trained (innate) immunity meaning you won't have any HERV-K102 activity to promote your survival should you become infected. However, anti-inflammatories are useful if you have cytokine storm. Interestingly, methylprednisolone (a type of corticosteroid which is anti-inflammatory) likely induces HERV-K102 expression while dexamethasone (a more powerful corticosteroid) likely blocks HERV-K102 expression and explains why more lives are spared from severe COVID-19 when methylprednisolone is used. Melatonin up to 2 mg per night is not going to inhibit trained innate immunity. Clinically we have observed that turmeric, statins and/or melatonin (>2 mg per night) worsen immunosenescence in the host and block the ability to achieve wellness. Our clinic (I am retired now from ISM) has been reversing and preventing immunosenescence in advanced cancer patients since 1998. Most herbal medicines are in fact immunosuppressive, so be careful. I hope this helps. Cannot discount the possibility for post vax sequelae that a short term exposure could help dissolve toxic spike. However, in the longer run it may be too dangerous to use immunosuppressives. Would like to see clinical trials on the use of low dose aspirin (antiinflammatory and anticlotting) to prevent clots versus breakthrough infections evaluating the risk of death. Happy New Year to you also!