


Spike Toxicity in the UK Elder and Males from Alberta, Canada
July 29, 2022

It is hard to keep up with Jessica Rose when she prowls for incriminating data on COVID-19 poor vaccine safety. Yesterday morning she did not disappoint.
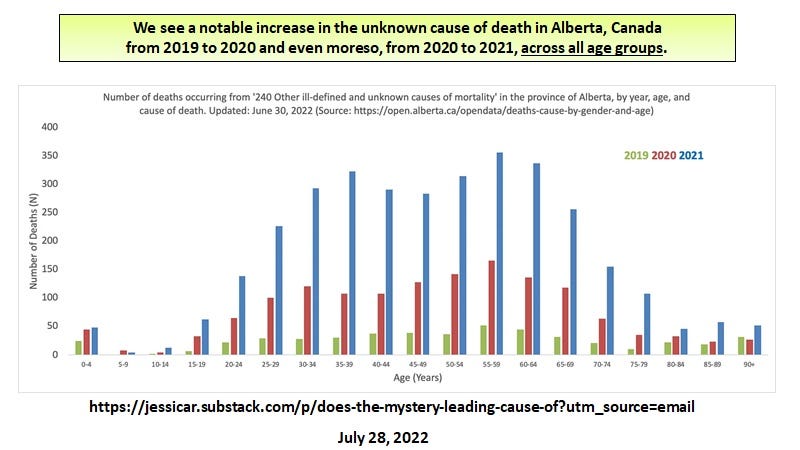
The day before, she alerted us to data showing the leading cause of death for 2021 in Alberta, a province in Canada, was “unknown”.
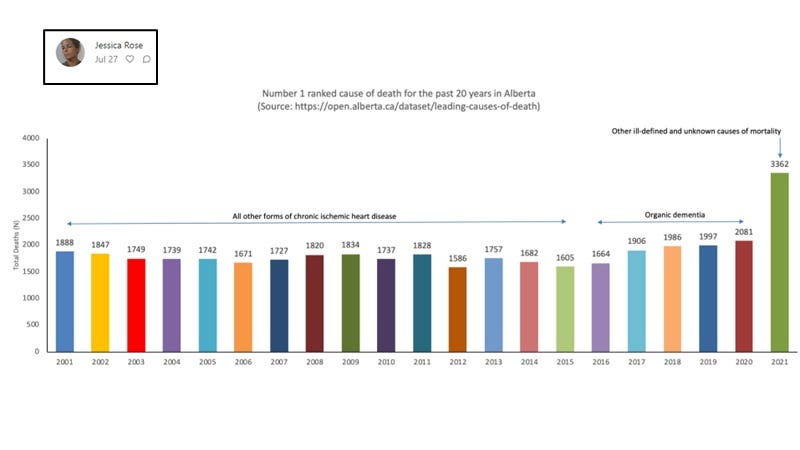
Image 1. Leading cause of death in Alberta, Canada was “unknown”. http://jessicar.substack.com/

In the slide deck below, it is argued that the evidence from the UK suggests that spike protein is toxic (death-inducing) in elder populations (particularly those in long term care facilities who may be more exposed to SARS-CoV-2 and more boosted). Additionally, from the exemplary work of Jessica Rose, it would appear that SARS-COV-2 infection but moreso, the mRNA COVID-19 vaccines may be toxic (death-inducing) in all age groups but where males are more susceptible as shown for Alberta, Canada from 2019 to 2021 for a special category of cause of death; ‘unknown’.
From this and the VAERS data, there can be no doubt that the vaccines have killed significant numbers of people with a predilection for males. It is time to STOP the administration of the COVID-19 vaccines, even more urgent for the omicron specific spike vaccines.
But why were the warning signs not heeded?
Here are 10 good reasons why the COVID-19 vaccines should NEVER have been approved under the EUA by any of the global regulators.
There were and remain many controversies about the COVID-19 mRNA vaccines, that should have stopped their use from the get-go.
First, before making a vaccine, let alone the approval under EUA, one must know what the immune correlate of protection is. This was not known at the time and indeed, it is only recently that a candidate critical immune correlate was identified [1]. Of course, it ended up being innate and not adaptive.
Second, from the get-go, it was well established that the antibodies and neutralizing antibodies correlated with progression and not protection during SARS-CoV-2 natural infection [reviewed in 1]. The three rogue papers claiming otherwise have been refuted, despite being published in high profile journals [1]. Why in the world would someone want to stimulate disease progression factors rather than immune protector mechanisms as a vaccine and during a deadly pandemic?
Third, a problem with antibody dependent enhancement (ADE) of infection was VERY strongly ANTICIPATED which historically prevented the successful development of safe and efficacious vaccines to a number of emerging or pandemic RNA viruses, for example, SARS-CoV-1 and HIV-1. ADE refers to antibodies and neutralizing antibodies to the receptor binding protein (here spike protein), which facilitate the abnormal entry of the virus into macrophages, promoting the progression of the disease. Macrophages are central to both innate and adaptive immunity. Wipe them out and frankly the whole immune surveillance goes out the window. There were many conflicting in vitro reports on the existence or biological outcomes of ADE for SARS-CoV-2 [reviewed 1]. In reality, though, by mid-to-late 2021, all the publications reported that in vivo, in severe and critical disease, the macrophages were productively infected by SARS-CoV-2 [1] but not before. At autopsy, all the macrophage subtypes in lung were variably productively infected [2].
_________________________________________
Interestingly, Two Types of ADE for SARS-CoV-2
During the course of my investigation for the paper I was writing, I uncovered that there were two types of ADE potentially operating in COVID-19 patients [1]. One was in the upper respiratory tract (URT) which involved sebocytes which are specialized lipid body negative foamy macrophages ( LB-FMs) producing the protector HERV-K102 foamy virus particles. Here, pre-formed vaccinal (vaccine-induced) neutralizing antibodies to spike protein could select for immune escape variants, and being in the URT, these selected variants could be transmitted. The ADE appeared to involve classical FCGR2A mechanisms [4] but did not involve BSG as the sebocytes downregulated BSG upon their activation (since they constitutively produce and release the HERV-K102 particles by lysis and where the sebum containing the released protector particles coats the mucosa [5]).
On the other hand, in the lower respiratory tract, there was a NOVEL type of ADE where associated with progression (ie., the concomitant development of spike specific and neutralizing antibodies released from plasma cells), there was a switch from spike:ACE2 (the primary receptor) to spike:BSG (the secondary receptor)[6] with apparently, no selection pressure.
Under most circumstances during natural infection there is little chance that selection of variants occurs in the URT because infectious virions after day 5 of the infection are rare and the adaptive antibodies are not generally triggered until after day 7 for 50% of the patients and after day 10 for 100% of the patients [7]. Indeed, there little to no evidence for the selection of the alpha or delta variants during the entire first year of the pandemic, except in countries that participated in the vaccine clinical trials such as the UK (see slidedeck). Moreover, evidence was convincingly demonstrated that in Canada, both the alpha and delta variants were selected following the administration of the second mRNA dose which strongly induced the neutralizing antibodies [1]. So the sole blame for the pandemic going on and on … and on, squarely rests with the second dose of the mRNA vaccines. And the manufacturers want to continue this charade while the middle class disappears with funneling of their resources to a select few manufactures?
___________________________________________
Fourth, even if the vaccine offered some protection against severe disease such as hospitalization and/or death (by activating and expanding the adaptive T cell response) which this one does, the neutralizing antibodies would provide selection pressure for the emergence of immune escape variants, meaning vaccination would prolong the pandemic. Furthermore, vaccination could NEVER achieve herd immunity, due to selection of immune escape variants. As such the infection rates per capita stratified by age were increased in the vaccinated over the unvaccinated in the UK with the delta variant confirming ADE-mediated infection. Thus, vaccination increased not decreased infection rates.
Fifth, it is no secret that there is a conundrum about vaccines. The need is to protect the most vulnerable, in this case the aged who: suffer immunosenescence, usually exhibit more than one comorbidity and who are often frail. However, vaccines do not work well in these populations. They are often tested in much younger, healthier individuals, but this misses the point.
Sixth, the mRNA vaccines represent a new technology… actually gene therapy with no proven safety profile [3]. The manufacturers did not provide even a year of human data addressing side-effects, laboratory indicators of effects on health, or even if the vaccines prevented hospitalizations and deaths. Moreover neither the manufacturers nor the regulators discussed the absolutely critical all-cause mortality assessment. We now know the mRNA vaccine spike protein lingers in the body for at least 60 days and many people suffered serious adverse events post-vaccination including death [3 and see slidedeck].
Seventh, the spike protein is perhaps the most toxic of the viral antigens. Its use as the primary or sole immunogen, helps to explain the avalanche of serious vaccine side effects including death noted in VAERS which was not seen in the entire existence of VAERS’s history [3].
Eighth, how does anyone recommend any vaccine with an unproven and highly suspect safety record to anyone or how does such an intervention achieve EUA? or regulatory FDA approval? How is this possible, especially when the critical all-cause mortality analysis in one instance indicated the vaccine caused more (all-cause) deaths than the placebo! (Now that’s a first!)
Nineth, how does anyone mandate a gene therapy under the guise of a vaccine with unproven safety to anyone? How do you mandate a vaccine on the premise that it is needed to establish herd immunity when you know the infection rates are higher per capita in the vaccinated when compared with the unvaccinated? In other words, the mandated approach destroys herd immunity yet the mandate premise is to establish herd immunity? How does this make any sense?
Tenth, how does one recommend/mandate an ‘experimental gene therapy’ (vaccine) when the risks versus benefits have not been addressed let alone established and no true informed consent is possible?
For the above 10 good reasons, these vaccines should not have been approved for EUA at the get-go. (Having worked in biological product approval at Health Canada, I find this particularly appalling.)
Let us not get complicit about the upcoming omicron specific vaccines. It is a clearly foreseeable disaster in the making.
We have to stop it now.
We have to focus on prevention and early intervention with well established and safe protocols [8,9].
Even the RCTs for repurposing the existing trained innate immunity vaccines (eg., the BCG vaccine) were sabotaged by the COVID-19 vaccine manufacturers [1].
Bring on the ivermectin and hydroxychloroquine!
Laderoute MP. Trained immunity involving HERV-K102 activation may promote recovery from COVID-19 providing a new vaccination paradigm against pandemic RNA viruses. Submitted: July 26, 2022.
Delorey TM, Ziegler CGK, Heimberg G, Normand R, Yang Y, Segerstolpe Å, et al. COVID-19 tissue atlases reveal SARS-CoV-2 pathology and cellular targets. Nature. 2021 Jul;595(7865):107-113. doi: 10.1038/s41586-021-03570-8.
Seneff S, Nigh G, Kyriakopoulos AM, McCullough PA. Innate immune suppression by SARS-CoV-2 mRNA vaccinations: The role of G-quadruplexes, exosomes, and microRNAs. Food Chem Toxicol. 2022 Jun;164:113008. doi: 10.1016/j.fct.2022.113008.
Ziegler CGK, Miao VN, Owings AH, Navia AW, Tang Y, Bromley JD, et al. Impaired local intrinsic immunity to SARS-CoV-2 infection in severe COVID-19. Cell. 2021 Sep 2;184(18):4713-4733.e22. doi: 10.1016/j.cell.2021.07.023.
Nelson AM, Zhao W, Gilliland KL, Zaenglein AL, Liu W, Thiboutot DM. Neutrophil gelatinase-associated lipocalin mediates 13-cis retinoic acid-induced apoptosis of human sebaceous gland cells. J Clin Invest. 2008 Apr;118(4):1468-78. doi: 10.1172/JCI33869.
Ren X, Wen W, Fan X, Hou W, Su B, Cai P, et al. COVID-19 immune features revealed by a large-scale single-cell transcriptome atlas. Cell. 2021 Apr 1;184(7):1895-1913.e19. doi: 10.1016/j.cell.2021.01.053.
Wölfel R, Corman VM, Guggemos W, Seilmaier M, Zange S, Müller MA, et al. Virological assessment of hospitalized patients with COVID-2019. Nature. 2020 May;581(7809):465-469. doi: 10.1038/s41586-020-2196-x.
McCullough PA, Alexander PE, Armstrong R, Arvinte C, Bain AF, Bartlett RP, et al. Multifaceted highly targeted sequential multidrug treatment of early ambulatory high-risk SARS-CoV-2 infection (COVID-19). Rev Cardiovasc Med. 2020 Dec 30;21(4):517-530. doi: 10.31083/j.rcm.2020.04.264.
Kory P, Meduri GU, Iglesias J, Varon J, Cadegiani FA, Marik PE. "MATH+" multi-modal hospital treatment protocol for COVID-19 infection: clinical and scientific rationale. J Clin Med Res. 2022 Feb;14(2):53-79. doi: 10.14740/jocmr4658.
I am struggling through RFK Jr's "The Real Anthony Fauci" this month. The explanation for approval is very well detailed. Follow the money.
If you constructed a Venn diagram including the WEF, the WHO, the Gates Foundation, major Pharma companies, and whichever other players you cared to include, you would find the intersections include most of the Vaxx pushers.
Recall that Teresa Tam is on the WHO "Pandemic Planning Committee." I now understand its "planning " function, and I don't believe it is mitigation. Note that our "leaders" are WEF minions, the "Schwab Youth" including Justin Trudeau, Chrystia Freeland, Jagmeet Singh, John Horgan here in BC, and others.
I would have loved to have had you as an immunology instructor, although I appreciate that you weren't at your present expertise during my brief course in the late 1970's. Thank you for the review and clear explanations.
Reference 1 is cited several times in your post. Where can we read it?