
On the Negative Effectiveness of COVID-19 "Adaptive Immunity" Vaccines in England
Risk-Benefit Profile on Multiple-dose mRNA Vaccines Might Not Justify Their Use

Updated March 25, 2022
Response to video posted February 4, 2022 on bitchute.com by Uncensored Doctors https://www.bitchute.com/video/256KlyHOlxJV/.
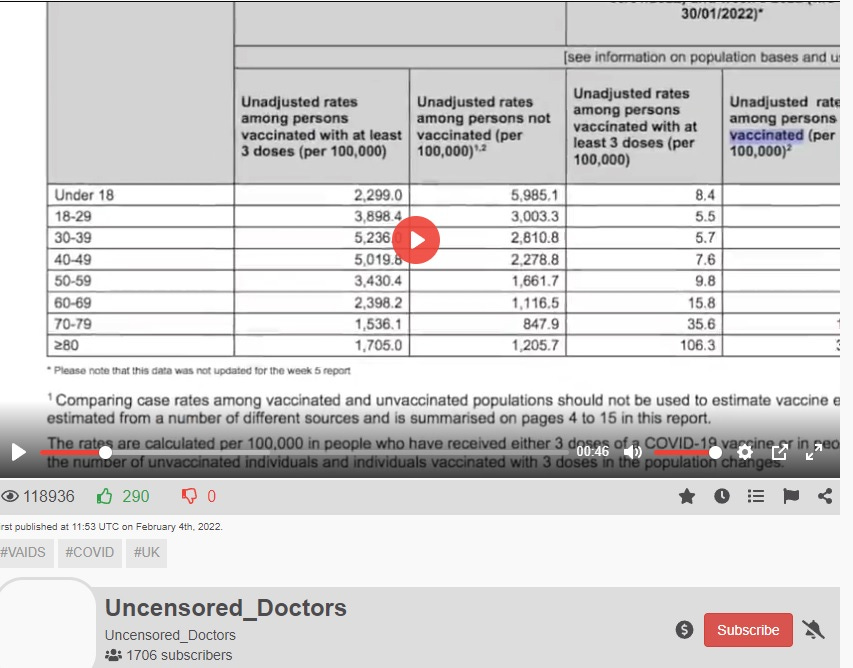
Image 1. Omicron Specific Infection Rate DATA from UKHSA Referred to In the Uncensored Doctors’ Post
Posted Feb 8 2022 RE Negative Effectiveness data from UKHSA by uncensored doctors
This data (Image 1) from UKHSA (which they no longer plot in graphs due to its damaging message) shows the vaccines are promoting COVID-19 infections. This means the vaccines cannot be used to promote herd immunity to end the pandemic. However induction of herd immunity is the scientific basis for the mandates.
Most likely the increased risk of infection is reflective of ADE (antibody dependent enhancement) of infection. Thus, these data invalidate the science behind the mandates. Moreover this has been apparent since delta emerged by June 2021 in the UK (Image 2). We see in Image 3 plotted for Canada and the US, that the vaccines have been selecting for higher transmission variants. Accordingly, the vaccines and their mandates should have ENDED (or not begun) since the onset of the delta variant for each of the countries (roughly mid 2021).
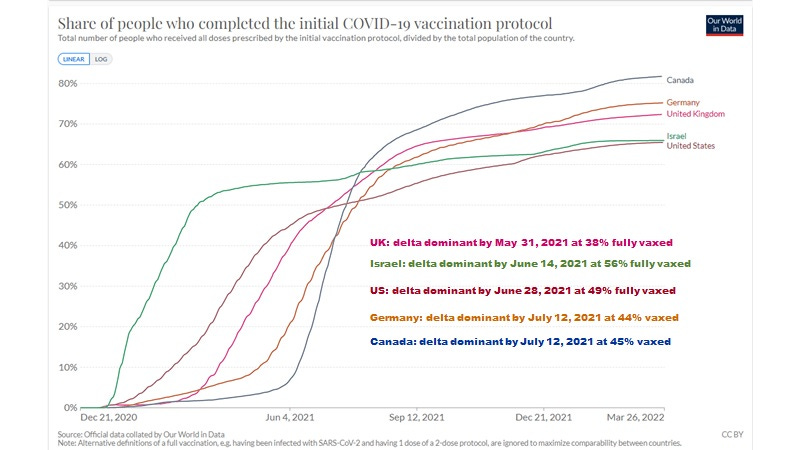
Image 2. Delta became dominant in the UK by May 31, 2021 at 38% fully vaxed.

Image 3. R value plots for Canada and United States Shows a Clear Trend for Increased Transmission of SARS-CoV-2 Due to Adaptive Immunity Vaccination
Surely the goal of adaptive immunity mass vaccinations was not to increase rates of transmission of SARS-COV-2.
Disturbing Trends on the Delta Variant Revealed
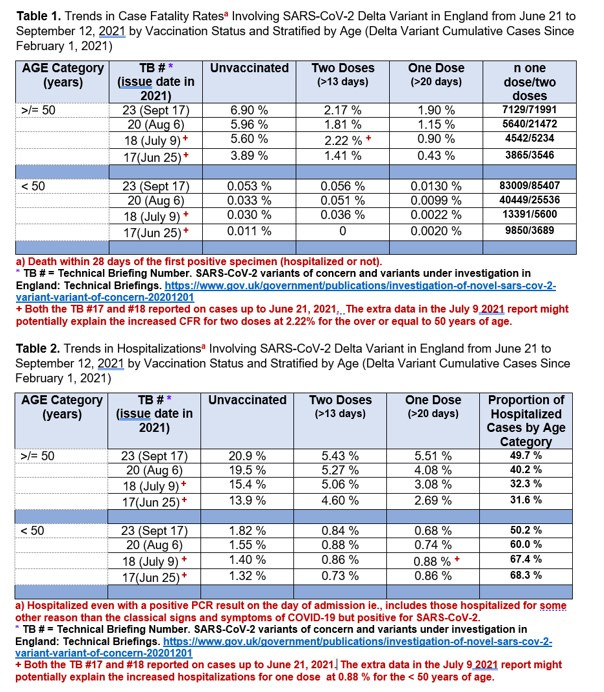
Image 4. Delta-variant Specific DATA from Technical Briefings from UKHSA
If we examine the Technical Briefing delta-specific data from week 17 (June 25) to week 23 (Sept 17) as posted at hervk102@substack.com (Image 4) we see evidence of a number of disturbing trends.
First, for both mortality and hospitalization as stratified by age, we see that as delta variants are being selected for by the vaccinal spike specific antibodies, there is a clear increase in pathogenesis with time (over a matter of weeks/months), including for the under 50 years of age category.
Surely the goal of adaptive immunity vaccination was not to increase rates of hospitalizations and deaths with time associated with the selection of variants.
Second, it is striking that in nearly all cases the least amount of mortality and hospitalization was associated with one dose of vaccine when compared with two doses or the unvaccinated. One mRNA dose appears to promote innate immunity mechanisms while it is only the two doses that significantly stimulates adaptive immunity spike specific antibodies and neutralizing antibodies (Jackson LA et al., NEJM July 14, 2020 and Walsh EE et al., NEJM Dec 17,2020).
So while there is some benefit of 2 doses of vaccine (adaptive immunity vaccination) over the unvaccinated for hospitalization and mortality especially in the 50 years of age and older, it is very clear that when compared to one dose innate immunity vaccination, two doses are causing hospitalizations and deaths (see attachment below for calculations of risks).
Surely the goal of adaptive immunity vaccination was not to cause hospitalizations and deaths.
Third, the benefits of two doses (adaptive immunity vaccination) are almost negligible for people under the age of 50. Indeed for deaths we see more deaths in those who received the 2 dose adaptive immunity vaccines than the unvaccinated.
Surely the goal of adaptive immunity vaccination was not to cause deaths in the under 50 years of age.
Roughly from Image 3, for delta related deaths, for every 2 deaths prevented there may be one death caused (50%) whereas for every 10-15 delta hospitalizations prevented there may be 1-2 caused (7-20%). This risk-benefit analysis would not support the approval of the COVID-19 vaccines even under EUA at least for the time that delta was circulating and thereafter.
Surely the goal of adaptive immunity vaccination was not to have higher risk-benefit ratios for pandemic responses (more harm than good).
Considering that evidence of serious adverse events associated with two doses of the vaccine were readily apparent by June 25, 2021 (Image 4), one has to question why these vaccines were not immediately taken off the market on June 25, 2021.
Indeed, worldwide, the selection for and emergence of the delta variant corresponded to a window where about 38% to 56 % of the population were administered the second dose of the vaccine (Image 2).
Surely the goal of adaptive immunity vaccination was not to select for SARS-CoV-2 immune escape mutants rendering the vaccine less potent and with ADE, more dangerous.
An in depth analysis for selection of the alpha and delta variants in Canada has been provided in this hervk102.substack.com article;

which showed when the two dose to one dose ratio for the population being vaccinated exceeded the 0.5 threshold, or when there was a notable loss in heterologous protection against death by one dose of the vaccine (as measured by a loss in negative excess all cause mortality), there was the emergence or dominance of the alpha or delta variants.
Here, heterologous protection against death from the one dose of vaccine refers to the antigen non-specific protection by trained innate immunity against intracellular pathogens and tumors. However because the release of the HERV-K102 particles from foamy sebocytes in the oral mucosa and from foamy monocyte/macrophages in the tissues by definition reverses immunosenescence, this heterologous protection then also includes protection against all causes of death (heart disease, cancer, diabetes, metabolic syndrome, autoimmune diseases, allergies and so on) because immunosenescence is known to cause these chronic diseases.
Surely the goal of adaptive immunity vaccination was not to abolish or weaken trained innate immunity, the first line of defense against any pathogen, and critical for host defense against emerging RNA viruses (as it cannot select for variants as it does not recognize virus specific antigens).
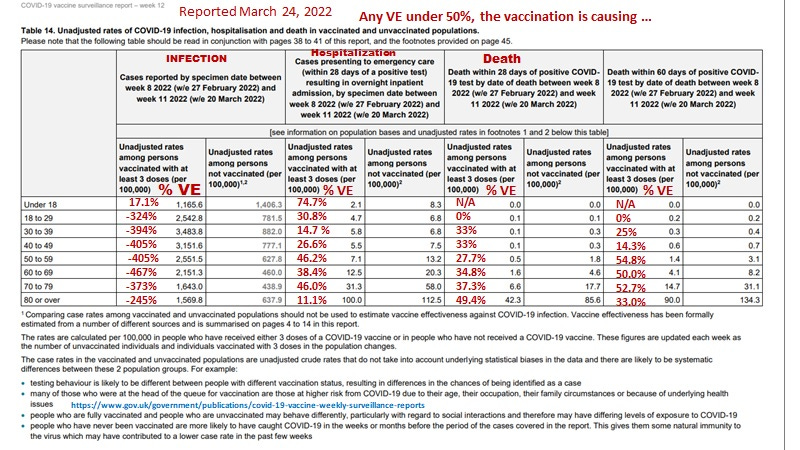
Image 5. The latest report from UKHSA indicates vaccination/boosting is causing the vast majority of symptomatic infections, the vast majority of hospitalizations (18 years of age and up) and vast majority of day 28 deaths (18 years of age and up).
More disturbing than the data in Image 4, are the current results for the UK as shown in Image 5, and reported March 24, 2022 where the majority of infections, hospitalizations (excluding the under 18 years of age) and death by 28 days after a positive SARS-CoV-2 test, can be ascribed to having received the third dose of adaptive immunity vaccine.
Surely the goal of adaptive immunity boosting was not to significantly cause increased symptomatic infections, to cause increased hospitalizations, or to cause increased deaths by 28 day (after a positive SARS-CoV-2 test).
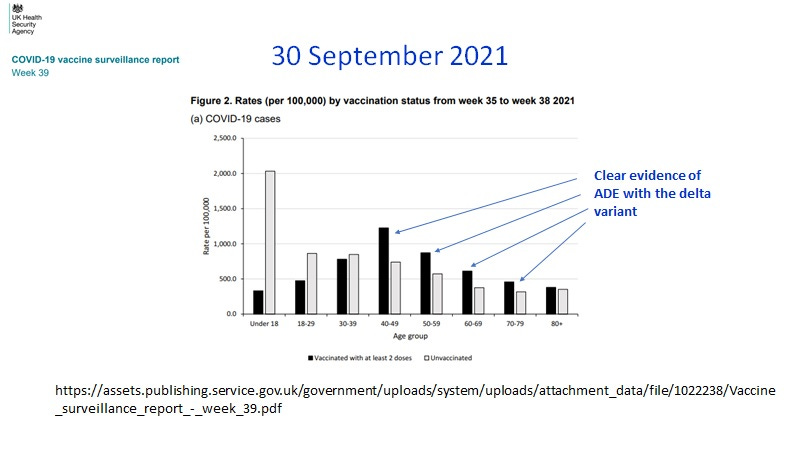
Image 6. Clear evidence of ADE with the delta variant published by UKHSA on 30 September 2021. (It is strongly suspected that evidence of ADE occurred earlier upon selection by the vaccines for the delta variant in the older age groups, but this critical data was not published).
Moreover, the UKHSA published on September 30, 2021 that the UK had clear evidence of ADE associated with the delta variant (Image 6), which undoubtedly occurred earlier in the older age groups but which was not reported.
Surely the goal of adaptive immunity vaccination was not to induce ADE and the known and expected associated increased transmission and pathogenesis.
The above data clearly indicates that by June 25, 2021 (Image 4) there was sufficient data to abort the “adaptive immunity vaccination program” in the United Kingdom, in order to prevent the totally predictable ‘catastrophic’ serious adverse event results shown in Image 5.
In total the above troubling statistics, strongly indicate that adaptive immunity vaccination during a pandemic was at best, ill-advised.
Advice Given During the Pandemic
If adaptive immunity vaccination was promoted as the only medical intervention for dealing with the pandemic, one has to ask who and what advice was being circulated at the time.
The inappropriateness of adaptive immunity vaccination against an RNA pandemic virus was vehemently voiced by the vaccinologist, Dr. Geert Vanden Bossche (see www.voiceforscienceandsolidarity.org) who warned against adaptive immunity vaccination since the onset of the pandemic. He continues to warn about these dire consequences, and how catastrophic an omicron-specific vaccine would be. This remains a huge concern as big Pharma rolls out its omicron specific vaccination clinical trials.
It was quite revealing, that the White House, despite the most qualified medical advisors in the world and supposedly the highest level of ‘intel’ for homeland security, did not anticipate the emergence of the more deadly delta variant with adaptive immunity vaccination as inadvertently admitted around December 18, 2021 [https://www.theguardian.com/us-news/2021/dec/18/kamala-harris-la-times-interview-covid-variants-vaccines].
One can only surmise what other truths Dr. Anthony Fauci did not inform the White House about.
For example what about early treatment with ivermectin which would have been far safer, more cost-effective, and would have abolished entirely the need for lock-downs. Ivermectin use would have prevented the ensuing collateral economic damage and societal injuries, not the least of which involved suicides, drug overdosing, loss of schooling, breakup of families, division and strife based on who was vaccinated or not and the loss of employment, and so on. Moreover, ivermectin with an unrivaled 30 year safety history and considered a ‘miracle drug’ (as it promotes overall wellness), unlike adaptive immunity vaccination would not cause
an increase in SARS-CoV-2 transmission rates,
selection for more pathogenic variants (or variants of any kind),
more hospitalizations (actually decreases),
the loss or weakening of trained innate immunity (actually enhances),
significant morbidity and mortality with or without SARS-CoV-2 co-infection (actually prevents morbidity and mortality of SARS-CoV-2 infection and enhances wellness in those not infected).
Indeed a review of the emerging evidence demonstrating the efficacy and effectiveness of ivermectin in the prophylaxis and treatment of COVID-19 published by March/April 2021 by Dr. Pierre Kory et al (American Journal of Therapeutics, 2021), and a separate review by the British Ivermectin Recommendation Development Panel clearly supported the widespread use of ivermectin for early intervention against COVID-19 morbidity and mortality. However, this truth was censored by those with an agenda to profit from adaptive immunity vaccination.
Clearly the White House was not informed by Dr. Fauci that it was considered highly unlikely that an adaptive immunity vaccine could be safe or effective against an emerging RNA pandemic virus. For example, there is yet no safe vaccine against epidemic SARS-CoV-1 or pandemic HIV-1, despite the passage of decades (17 years and 37 years respectively). Indeed, after the reports of increased transmission of HIV-1 in vaccinees from the STEP HIV-1 vaccine trial, these concerns led Dr. Fauci as Director of the NIAID to lead a summit in March 2008 to provide new directions in HIV-1 (pandemic) vaccine research (Bradac J & Dieffenbach CW. HIV vaccine development: Lessons from the past, informing the future. IDrugs 2009). Clearly Dr. Fauci had hand-on experience that adaptive immunity vaccines not only did not work, but were dangerous. Yet, this information was not communicated to the President and Vice-President of the US.
The medical literature in 2020 but hardly thereafter due to censorship promulgated largely by big Pharma, the Gates Foundation and the NIH, had warned about the well documented concern about antibody dependent enhancement (ADE) of infection and and the risks associated with enhanced infection, morbidity and mortality in those fully vaccinated against an emerging pandemic RNA virus. Of these, the article by Lee WS et al (Antibody-dependent enhancement and SARS-CoV-2 vaccines and therapies. Nature Microbiology, October 2020) was the most poignant. It gave us a very important clue; that one could expect serious problems with adaptive immunity vaccines against SARS-CoV-2 given that antibodies and neutralizing antibodies have been correlated with severity rather than protection during natural infection with SARS-CoV-2!
Where are we now?
Fortunately, the mass (adaptive immunity) vaccination coordinated by big Pharma and the Gates Foundation, and implemented by captured agencies and governments (WHO, NIH, CDC, FDA, Health Canada, Public Health Agency of Canada; and so on) did not extend into non-human, wild animal populations. Out of the blue, omicron has emerged; perhaps from the common house mouse (Wei C et al., J Genet Genom 2021). Some have heralded omicron as an attenuated 'endemic' vaccine which has potential to end the pandemic (Po ALW. J Clin Pharm Thera, 2022).
An analysis on whether omicron could provoke protection to end the pandemic was recently posted at hervk102.substack.com:
which has shown the temporal return of negative all cause mortality associated with widespread infection by omicron interestingly for some countries but not others.
Accordingly, as long as big Pharma does not introduce an omicron specific vaccine (which is predicted to restart the pandemic), hopefully omicron will have overcome the devastating harm generated by mass adaptive immunity vaccination.
Notes added after posting.

Image 7. USA-Derived Evidence for Diminishing VE of Adaptive Immunity Vaccination Against Infection but Not For Innate Immunity Vaccination Over Time
In Image 7, we see that in the USA (California) for the over 64 years of age population that the infection VE of two doses (greater than 6 days after the second dose) diminishes from 84% in March 2021 to about 44 to 48 % by July-August 2021 associated with the emergence and evolution of the delta variant.
Nevertheless, during the same time, with the emergence of the alpha and delta variants, we see that at under 7 days following the second dose, there is 100% VE against infection. These results are consistent with the notion that boosting trained innate immunity may provide sterilizing immunity against SARS-CoV-2 selected variants.
Thus, these results along with the data from England in Image 4, suggest innate immunity vaccination and boosting protocols (for example, 1st dose mRNA and 2nd dose the BCG trained innate immunity vaccine, Arts RJW et al., Cell Host Microbe, 2018) may provide a better approach to controlling and ending RNA virus pandemics than the use of adaptive immunity vaccines. The latter generate neutralizing antibodies and other receptor binding domain antibodies capable both of selection for variants and subsequently mediating ADE. These findings suggest that innate immunity vaccines which do not select for variants as they do not recognize pathogen specific antigens, could be prioritized for future pandemics at least for the most at risk PROVIDED THEY ARE WELL ESTABLISHED TO BE SAFE AND THAT IMMUNOSENESCENCE IS FIRST REVERSED IN THE MOST AT RISK BEFORE THE VACCINE IS ADMINISTERED.
From the calculations (see attached) in the >49 years of age, 1/123 deaths due to the delta variant were caused by the second dose of vaccine (average difference between 2 doses and 1 excess deaths of 0.81%). For the hospitalizations about 1.69% could be ascribed to the administration of the second dose or about 1/59. I verified that there were deaths and hospitalizations during the May 28 to September 10, 2021 time frame.
With these extraordinary numbers and adverse effects including deaths, we are left with many important questions. Why did the UK continue to administer two doses of COVID-19 vaccines and then boosters after June 25 2021? Why did Dr. Fauci not intervene when he knew full well that ADE was expected and then observed for adaptive immunity vaccination upon selection of the delta variant (the earliest in the UK) by these vaccines? Who exactly were asleep at the wheel and what exactly caused them to dose off?
More importantly, where are the corresponding data for Canada and the US?
Of course, all the above strongly supports the priority testing for HERV-K102 particle production, proviral genomic integration (conducted on genomic DNA sloughed into plasma), HERV-K102 envelope specific antibody and T cells in the prevention and recovery from SARS-CoV-2 infections particularly since increased proviral genomic integration was associated with sterilizing immunity for another RNA virus pandemic virus, HIV-1 (Laderoute M et al., Open AIDS J, 2015).
In order to reduce the risk of immunosenescence in causing vaccine-related morbidity and/or mortality, vaccine recipients should be screened for immunosenescence and treated prior to administration of vaccines. These high risk individuals should receive this treatment for the duration of the pandemic. Protocols might use zinc and flavonoids in simple cases whereas others may need additional alpha-fetoprotein antagonists (Laderoute M, Discovery Medicine, 2015, 2020). Screening for immunosenescence could be as simple as blood pressure measurements.