

By Late June of 2021 in England, There Were Early Warning Signals of mRNA COVID-19 Vaccine Harm
By Late June of 2021 in England, There Were Early Warning Signals of mRNA COVID-19 Vaccine Harm
August 19, 2022

Pandemic RNA viruses differ from traditional viruses in that they are recently emerged and have not yet had the time to reach 'endemic status'. As explained by Lythgoe et al., [1] if there are no selective pressures put on the pandemic RNA virus, the virus will naturally evolve to one with higher transmission and less pathogenesis. Eventually, the virus will reach a state of balance referred to as endemic status (taming). However, if there are selective pressures such as neutralizing antibodies (NAbs), these antibodies will select for more transmissible variants (no longer neutralized by the NAbs, thus escape mutants) with higher virulence.
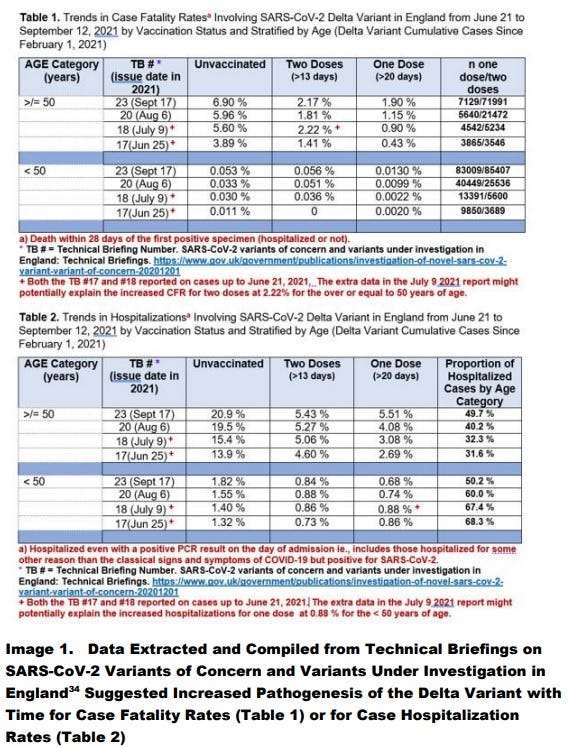
As can be seen in Image 1, by June 25, 2021 from Technical Briefing # 17 in England, we see evidence in the 50+ that one dose of the vaccine provided better protection against delta variant mortality than two doses. In fact we can say that the second dose appeared to be causally associated with the induction of at least 1% mortality rate over those only inoculated with one dose. Note that in the unvaccinated the case fatality rates increased over time (as well as in the one dose and two dose vaccinated). This was expected as predicted by Lythgoe et al [1].
While the first dose of the mRNA vaccines provides innate immunity protection against SARS-CoV-2 associated with heterologous protection against COVID-19 mortality (Image 1) and non-COVID-19 mortality [2], it is the second dose of mRNA vaccine which significantly produces spike specific antibodies including the neutralizing antibodies [3 - 5], which selects for more pathogenic variants (Image 1).
As shown in Image 2, as expected, breakthrough infections in people who were fully vaccinated (2 doses) showed higher levels of immune escape variants and/or more infectious variants, when compared with the unvaccinated whereas the people who received only one dose showed the least amount of selection for antibody resistant and more infectious strains [6].
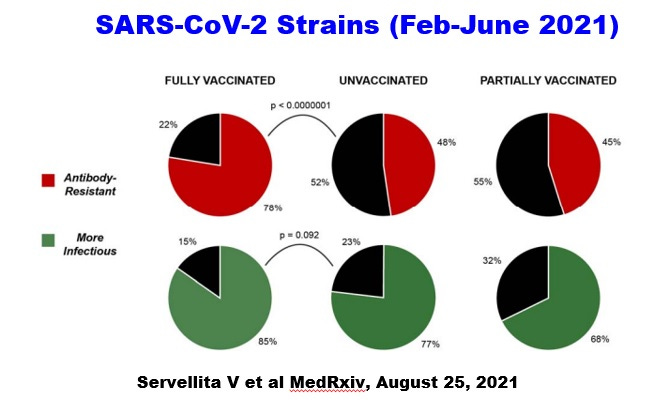
Image 2. Evidence that the second dose selects for immune escape variants and/or more infectious strains when compared with unvaccinated and those who received only one dose.
Indeed in a study conducted in Ontario, Canada, the alpha variant was more virulent than the original Wuhan strain, while the delta variant was more virulent than the alpha strain [7]. This showed that with selection due to neutralizing antibodies, the mass vaccination with two doses of mRNA vaccines, caused increased virulence as predicted by Lythgoe et al in 2013. [1].
It should also be noted that in Canada, evidence was presented suggesting that it was the second dose of the mRNA vaccines that selected for the alpha and then the delta initial emergence and then their dominance [8,9].
Finally, it should be noted that unlike SARS-CoV-1 which was a direct zoonotic transmission to humans in 2002, SARS-CoV-2 emerged in 2019-2020 as fully adapted to humans [10] and not as a direct zoonotic transmission [11]. The direct evidence for this was the demonstration of the selection of immune escape variants for SARS-CoV-1 in the first few months of this pandemic but NOT with SARS-CoV-2 [10]. Also SARS-CoV-2 uses multiple ways to circumvent the HERV-K102 trained (innate) immunity system. Since this protector system only exists in humans it means selection likely occurred through passage through humanized mice, especially the BLT mouse with a xenografted human fetal lung as discussed earlier [11].
The problems with exposing the truth on the highly sensitive topic that SARS-CoV-2 likely was accidently released from the Wuhan Institute of Virology itself provides an interesting story for Alina Chan [https://www.technologyreview.com/2021/06/25/1027140/lab-leak-alina-chan/]. Perhaps film-makers might want to make a movie about this.
The fact that SARS-CoV-2 emerged fully adapted to humans means that it had already hit ‘endemic status’ according to Lythgoe et al [1]. Thus, the proper response at the time of emergence of SARS-CoV-2 would have been to provide early and prophylactic treatment to stop the morbidity and mortality of SARS-CoV-2 [12,13] but more importantly to quench the pandemic as had been shown in the province of Uttar Pradesh in India [14]. The reason why the ivermectin based therapy which also used zinc, quercetin, Vitamin D etc., worked so well is that it reversed and prevented the immunosenescence (dysfunction) of the lipid body negative foamy macrophages (LB-FMs) which provides the critical trained (innate) immunity involving HERV-K102 particle production against pandemic RNA viruses [8,15]. The dysfunction or immunosenescence of LB-FMs is the critical risk factor for COVID-19 severity [8,15] as immunosenescence is causally related to chronic diseases [16] and one or more chronic diseases including symptoms such as hypertension and/or insulin resistance is well established to greatly enhance COVID-19 severity risks. Therefore by reducing the risk of severe disease and at the same time quenching the pandemic with these protocols, this approach could have averted the mortality and morbidity associated with SARS-CoV-2 infection or by the vaccines and ended the pandemic by early March 2021.
However, since the captured public agencies around the world seemed to be more concerned about making a profit than saving human lives, we are now entering the 7th wave, and they wish to prolong the pandemic by selecting for omicron variants with the newer omicron specific vaccines where it is known safety issues would not have been addressed prior to EUA.
As mentioned by early 2022 the pandemic had evolved from SARS-CoV-2 excess mortality to vaccine induced excess mortality such that for the 2110 lives saved by mass vaccination in England, there was an excess of 423,337 deaths due to the toxicity of the gene therapy mRNA vaccines [17].
My question is how did Public Health England not see that the adaptive immunity vaccines were selecting for more virulent variants and/or that the vaccines were obviously harmful, given that they generated the data provided in Image 1 and made it available as early as June 25, 2021?
It should be noted that not long after I posted Image 1 on LinkedIn on Friday October 1, 2021, I received a comment from Ian Culbert, the Executive Director of the Canadian Public Health Association on Tuesday October 5th, 2021 shaming me and threatening me that LinkedIn should block my account for promoting vaccine hesitancy. On Tuesday October 26, 2021 at 1 o’clock pm, I was banned from LinkedIn and lost communication with over 7,800 followers most of whom were scientists and clinicians concerned about the COVID-19 pandemic and the direction it was taking.
Thus, the early warning data was censured by LinkedIn and now we have people being directly killed by the experimental mRNA vaccines but without their informed consent. This is what the censorship by the NIH and others including the Canadian Public Health Association paid for, backed by $$ from Big Pharma.
REFERENCES:
Lythgoe KA, Pellis L, Fraser C. Is HIV short-sighted? Insights from a multistrain nested model. Evolution. 2013 Oct;67(10):2769-82. doi: 10.1111/evo.12166.
Xu S, Huang R, Sy LS, Glenn SC, Ryan DS, Morrissette K et al. COVID-19
vaccination and non–COVID-19 mortality risk — seven integrated health care
organizations, United States, December 14, 2020–July 31, 2021. MMWR
Morb Mortal Wkly Rep 2021;70:1520–1524.
doi: http://dx.doi.org/10.15585/mmwr.mm7043e2.
Arunachalam PS, Scott MKD, Hagan T, Li C, Feng Y, Wimmers F, et al. Systems vaccinology of the BNT162b2 mRNA vaccine in humans. Nature. 2021 Aug;596(7872):410-416. doi: 10.1038/s41586-021-03791-x.
Walsh EE, Frenck RW Jr, Falsey AR, Kitchin N, Absalon J, Gurtman A, et al. Safety and immunogenicity of two RNA-based Covid-19 vaccine candidates. N Engl J Med. 2020 Dec 17;383(25):2439-2450. doi: 10.1056/NEJMoa2027906.
Chu L, McPhee R, Huang W, Bennett H, Pajon R, Nestorova B, et al. A preliminary report of a randomized controlled phase 2 trial of the safety and immunogenicity of mRNA-1273 SARS-CoV-2 vaccine. Vaccine. 2021 May 12;39(20):2791-2799. doi: 10.1016/j.vaccine.2021.02.007.
Servellita V, et al., Predominance of antibody-resistant SARS-CoV-2 variants in vaccine breakthrough cases from San Francisco Bay Area, California. medRxiv, August 25, 2021. https://www.medrxiv.org/content/10.1101/2021.08.19.21262139v1
Fisman DN, Tuite AR. Evaluation of the relative virulence of novel SARS-CoV-2 variants: a retrospective cohort study in Ontario, Canada. CMAJ. 2021 Oct 25;193(42):E1619-E1625. doi: 10.1503/cmaj.211248.
Laderoute M. Trained immunity involving HERV-K102 activation may promote recovery from COVID-19 providing a new vaccination paradigm against pandemic RNA viruses. (submitted).
Laderoute M. Did the second dose of the mRNA COVID-19 vaccines select for the alpha and delta variants which prolonged the pandemic? hervk102.substack.com, June 30, 2022.
Zhan SH, Deverman BE, Chan YA. SARS-CoV-2 is well adapted for humans. What does this mean for re-emergence? bioRxiv, May 2, 2020. https://www.biorxiv.org/content/10.1101/2020.05.01.073262v1.
Laderoute M. COVID-19 Lab-Leak Hypothesis Gains Momentum. hervk102.substack.com. June 21, 2022.
Kory P, Meduri GU, Iglesias J, Varon J, Cadegiani FA, Marik PE. "MATH+" multi-modal hospital treatment protocol for COVID-19 infection: clinical and scientific rationale. J Clin Med Res. 2022 Feb;14(2):53-79. doi: 10.14740/jocmr4658.
McCullough PA, Alexander PE, Armstrong R, Arvinte C, Bain AF, Bartlett RP, et al. Multifaceted highly targeted sequential multidrug treatment of early ambulatory high-risk SARS-CoV-2 infection (COVID-19). Rev Cardiovasc Med. 2020 Dec 30;21(4):517-530. doi: 10.31083/j.rcm.2020.04.264.
Kory P, Meduri GU, Varon J, Iglesias J, Marik PE. Review of the emerging evidence demonstrating the efficacy of ivermectin in the prophylaxis and treatment of COVID-19. Am J Ther. 2021 Apr 22;28(3):e299-e318. doi: 10.1097/MJT.0000000000001377.
Laderoute M. Ivermectin may prevent and reverse immunosenescence by antagonizing alpha-fetoprotein and downmodulating PI3K/Akt/mTOR hyperactivity. Open Heart, April 29, 2021. https://openheart.bmj.com/content/8/1/e001655.responses#ivermectin-may-prevent-and-reverse-immunosenescence-by-antagonizing-alpha-fetoprotein-and-downmodulating-pi3k-akt-mtor-hyperactivity.
Laderoute MP. A new paradigm about HERV-K102 particle production and blocked release to explain cortisol mediated immunosenescence and age-associated risk of chronic disease. Discov Med. 2015 Dec;20(112):379-91.
Laderoute M. A New Pandemic 2022. hervk-102.substack.com, August 13, 2022.

Actually, if we look at the mortality data for JANUARY 2021 as released by the UK Office for National Statistics on July 6, 2022, for all ages, the vaccinated were at 1.3-fold increased risk of COVID-19 deaths over the unvaccinated while for the non-COVID-19 deaths the risk was 1.5-fold. For the last month reported, May 2022, the increased risks were 3.4-fold and 10-fold respectively. THE VACCINES SHOULD HAVE BEEN STOPPED BY EARLY FEBRUARY 2021. We have to ask why the vaccines continued in the UK after January 2021.
Congratulations for your hard work. Thanks for sharing. The truth will prevail.